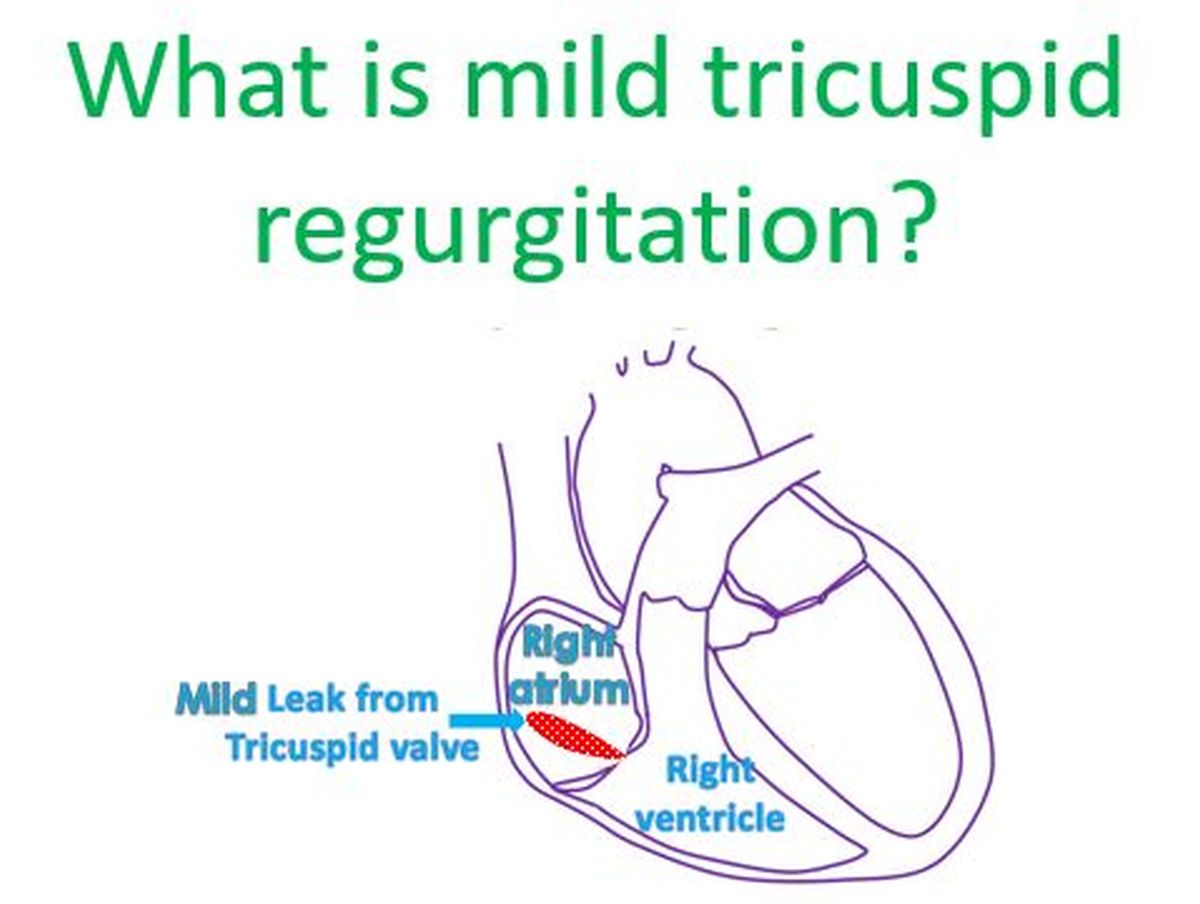
Mild tricuspid regurgitation (TR) is a common and often benign finding in cardiac imaging, particularly in echocardiography. It refers to a slight leakage of blood backward through the tricuspid valve from the right ventricle to the right atrium during ventricular contraction. While the term “regurgitation” might sound alarming, “mild” signifies a low grade of this backflow, which typically does not cause significant symptoms or require specific treatment. Understanding mild TR involves delving into the anatomy and function of the tricuspid valve, the mechanisms behind regurgitation, its prevalence, diagnostic approaches, and its generally favorable prognosis.
The Tricuspid Valve: Anatomy and Function
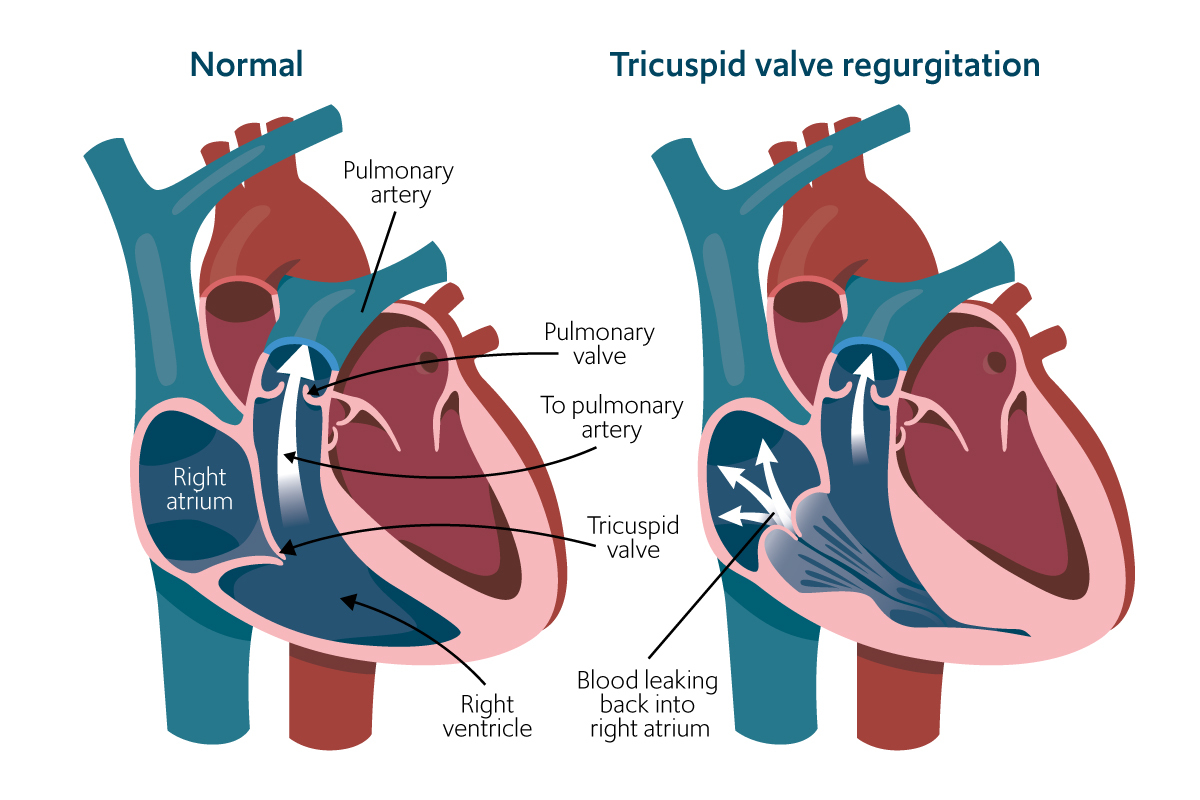
The tricuspid valve is one of the four main valves of the heart, strategically positioned between the right atrium and the right ventricle. Its primary role is to ensure unidirectional blood flow through the right side of the heart. Deoxygenated blood from the body returns to the right atrium and then flows through the tricuspid valve into the right ventricle. During ventricular contraction (systole), the tricuspid valve leaflets coapt, or close, preventing blood from flowing backward into the right atrium. The now-oxygenated blood is then pumped from the right ventricle to the lungs for oxygenation.
Anatomy of the Tricuspid Valve
The tricuspid valve is composed of three leaflets: the anterior, posterior, and septal leaflets. These leaflets are attached to the annulus, a fibrous ring that forms the valve’s structural base. Chordae tendineae, thin fibrous cords, extend from the edges of the leaflets to papillary muscles, which are muscular projections within the right ventricle. These chordae tendineae and papillary muscles play a crucial role in tethering the leaflets during ventricular contraction, preventing them from prolapsing backward into the right atrium.
Normal Tricuspid Valve Function
In a healthy heart, the tricuspid valve opens fully to allow unimpeded blood flow from the right atrium to the right ventricle during diastole (when the ventricle relaxes). As the right ventricle begins to contract, the pressure within the ventricle rises, causing the tricuspid valve to close effectively. This closure, aided by the synchronized contraction of the papillary muscles and the tension of the chordae tendineae, prevents any significant backflow of blood into the right atrium. The competence of the tricuspid valve is vital for maintaining the efficient pumping of blood through the pulmonary circulation.
Mechanisms of Tricuspid Regurgitation
Tricuspid regurgitation occurs when the tricuspid valve leaflets do not coapt properly, allowing blood to leak backward into the right atrium. This malcoaptation can arise from various issues affecting the leaflets themselves, the valve annulus, or the supporting structures like the chordae tendineae and papillary muscles.
Primary Tricuspid Regurgitation
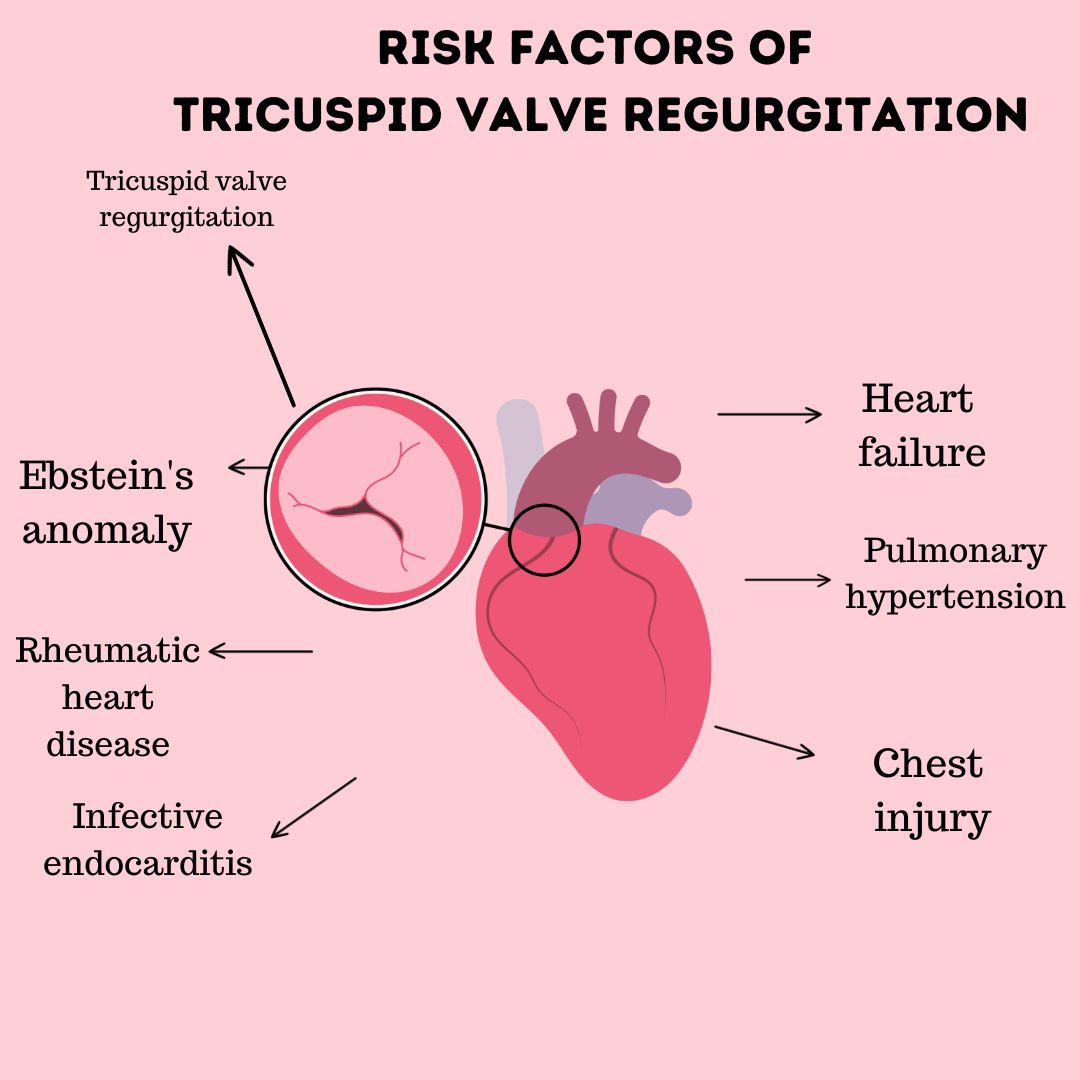
Primary TR, also known as organic TR, arises from intrinsic abnormalities of the tricuspid valve apparatus. This can include:
- Degenerative Valve Disease: This is a common cause, where the leaflets may become thickened, calcified, or myxomatous, leading to impaired closure.
- Rheumatic Heart Disease: While less common for tricuspid valve involvement than the mitral or aortic valves, rheumatic fever can cause leaflet thickening and fusion.
- Endocarditis: Infection of the heart valves can lead to vegetation formation and leaflet damage, impairing valve function.
- Congenital Abnormalities: Rare congenital defects can affect the structure of the tricuspid valve, predisposing to regurgitation.
- Trauma: Direct chest trauma can sometimes injure the tricuspid valve apparatus.
- Radiation Therapy: Radiation to the chest can lead to valvular damage over time.
Secondary (Functional) Tricuspid Regurgitation
Secondary TR, often referred to as functional TR, is a consequence of changes in the right ventricle or its annulus, rather than a primary problem with the valve leaflets themselves. This type of TR is far more common than primary TR. The primary drivers of functional TR include:
- Right Ventricular Dilation and Dysfunction: Conditions that lead to enlargement of the right ventricle, such as pulmonary hypertension, left-sided heart failure, or chronic lung disease, can stretch the tricuspid annulus. As the annulus dilates, the leaflets are pulled further apart, preventing effective coaptation.
- Pulmonary Hypertension: Elevated pressure in the pulmonary arteries increases the workload on the right ventricle. Over time, this can lead to right ventricular hypertrophy and dilation, which in turn causes annular dilation and functional TR.
- Left Ventricular Dysfunction: Severe left ventricular failure can lead to increased pressures in the left atrium, which can back up into the pulmonary veins and pulmonary arteries, causing pulmonary hypertension and subsequent right ventricular strain.
- Cardiac Surgery: Surgery on the mitral valve or septum can sometimes inadvertently affect the tricuspid valve apparatus, leading to TR.
- Pacemaker/ICD Leads: In rare instances, indwelling leads can cause leaflet restriction or dysfunction.
Diagnosis and Assessment of Mild Tricuspid Regurgitation
The diagnosis and assessment of tricuspid regurgitation, including mild TR, primarily rely on echocardiography, a non-invasive ultrasound imaging technique. Other diagnostic tools may be used for a comprehensive cardiovascular evaluation but are not typically the primary means of identifying mild TR.
Transthoracic Echocardiography (TTE)
Transthoracic echocardiography is the cornerstone for evaluating tricuspid regurgitation. It involves placing a transducer on the chest to visualize the heart’s chambers, valves, and blood flow.
- Visualizing the Valve: The echocardiogram allows for direct visualization of the tricuspid valve leaflets, assessing their structure, mobility, and any signs of thickening, calcification, or prolapse.
- Doppler Assessment: Color Doppler is crucial for detecting and quantifying regurgitation. It overlays the direction and velocity of blood flow onto the 2D image. A jet of blood flowing backward into the right atrium during systole indicates TR.
- Quantifying Severity: Echocardiography employs several parameters to assess the severity of TR, ranging from trivial to mild, moderate, and severe. For mild TR, specific findings include:
- Color Doppler Jet Area: A small, localized color Doppler jet area in the right atrium.
- Regurgitant Volume and Flow Area: Relatively small calculated regurgitant volumes and flow convergence areas.
- Hepatic Vein Flow: Normal or only mildly affected flow patterns in the hepatic veins.
- Inferior Vena Cava (IVC) Size and Collapse: The IVC is typically normal in size and shows significant collapse with inspiration.
- Right Ventricular Size and Function: The right ventricle is usually normal in size and function.
- Assessing Underlying Cause: Echocardiography also helps identify the underlying cause of TR, whether it’s primary valvular disease or secondary to right ventricular enlargement or pulmonary hypertension.
Transesophageal Echocardiography (TEE)
In certain situations, such as when transthoracic views are suboptimal or for more detailed assessment, transesophageal echocardiography may be performed. A transducer is passed down the esophagus, providing clearer images of the heart’s posterior structures, including the tricuspid valve.
Other Diagnostic Modalities
While not primary diagnostic tools for mild TR itself, other tests might be part of a broader cardiac workup:
- Electrocardiogram (ECG): Can reveal signs of right atrial enlargement or right ventricular strain if the TR is associated with more significant underlying heart disease.
- Chest X-ray: May show cardiomegaly (enlarged heart) or signs of pulmonary congestion in cases of more severe TR or underlying causes.
- Cardiac Magnetic Resonance Imaging (CMR): Offers highly accurate volumetric assessment of the right ventricle and precise quantification of TR, but is typically reserved for complex cases or when echocardiography is inconclusive.
- Cardiac Catheterization: An invasive procedure usually reserved for assessing coronary artery disease or complex congenital heart disease, but can also measure pressures in the cardiac chambers and pulmonary artery, which is indirectly related to TR severity.
Prognosis and Management of Mild Tricuspid Regurgitation
The prognosis for individuals diagnosed with mild tricuspid regurgitation is generally excellent, and it rarely requires specific medical intervention. The focus of management, if any, is on addressing the underlying cause, if present, and monitoring for any progression.
Prognostic Factors
The significance of TR is determined by its severity and the presence of any associated cardiac pathology. Mild TR, by definition, has minimal hemodynamic impact.
- Isolated Mild TR: When mild TR occurs in isolation, without any significant enlargement of the right ventricle or atrium, and with normal pulmonary artery pressures, it is considered hemodynamically insignificant. In such cases, the prognosis is essentially that of a normal healthy heart. These individuals do not typically experience symptoms related to the TR.
- Mild TR with Underlying Causes: If mild TR is present but associated with conditions like mild pulmonary hypertension or slight right atrial enlargement, the prognosis is still generally good, but it warrants attention to the underlying condition. The focus shifts to managing the primary cause.
- Progression of TR: While rare for mild TR to progress significantly on its own, it can occur if the underlying condition worsens. For example, if pulmonary hypertension progresses, it can lead to further right ventricular dilation and increased TR severity.
Management Strategies
For the vast majority of individuals with mild tricuspid regurgitation, no specific treatment is necessary.
- Observation and Monitoring: The primary approach is often periodic follow-up with echocardiography, especially if there is a known underlying condition that could potentially lead to TR progression. The frequency of monitoring is determined by the physician based on the individual’s overall cardiovascular health and the presence of any risk factors.
- Management of Underlying Conditions: If mild TR is secondary to another condition, such as hypertension, heart failure, or lung disease, the focus of treatment will be on managing that primary condition. This might involve medications, lifestyle modifications, or other therapies aimed at improving the overall health of the cardiovascular system.
- For Pulmonary Hypertension: If mild TR is related to pulmonary hypertension, treatments to lower pulmonary artery pressures are paramount. This can include medications like vasodilators or endothelin receptor antagonists, depending on the type and severity of pulmonary hypertension.
- For Heart Failure: If left-sided heart failure is contributing to secondary TR, management will focus on optimizing heart failure therapy, which may involve diuretics, ACE inhibitors, beta-blockers, or other heart failure medications.
- Lifestyle Recommendations: Maintaining a healthy lifestyle, including a balanced diet, regular exercise, avoiding smoking, and managing stress, is beneficial for overall cardiovascular health and can indirectly support the heart’s function.
- Surgical Intervention: Surgical intervention for tricuspid regurgitation is reserved for cases of moderate to severe TR that are causing symptoms or leading to significant right-sided heart dysfunction. Mild TR, by its nature, does not typically meet the criteria for surgical repair or replacement.
In conclusion, mild tricuspid regurgitation is a common echocardiographic finding that, in most instances, represents a minor physiological variation rather than a disease process. Its benign nature and excellent prognosis underscore the importance of accurate interpretation of echocardiographic findings and a comprehensive approach to cardiovascular health, focusing on the underlying physiology and individual patient factors.