The question of blood compatibility is a critical one, and understanding the nuances of blood types, particularly for Rh-negative individuals, is paramount for safe transfusions. While the direct answer to “what blood can a negative receive” might seem straightforward, a deeper dive reveals the complexities of the ABO and Rh systems, the vital role of antibodies, and the potential risks associated with incompatible transfusions. This exploration delves into the immunological principles that govern blood transfusions, ensuring patient safety and optimal treatment outcomes.
Understanding the ABO and Rh Blood Group Systems
Blood types are determined by the presence or absence of specific antigens on the surface of red blood cells. These antigens, along with corresponding antibodies found in the plasma, form the basis of the ABO and Rh blood group systems, the most important in transfusion medicine.
The ABO System: Antigens and Antibodies
The ABO system classifies blood into four main types: A, B, AB, and O.
- Type A: Individuals have A antigens on their red blood cells and anti-B antibodies in their plasma.
- Type B: Individuals have B antigens on their red blood cells and anti-A antibodies in their plasma.
- Type AB: Individuals have both A and B antigens on their red blood cells but no anti-A or anti-B antibodies in their plasma. This makes them universal recipients within the ABO system.
- Type O: Individuals have neither A nor B antigens on their red blood cells but have both anti-A and anti-B antibodies in their plasma. This makes them universal donors within the ABO system.
The presence of antibodies is crucial. If a person receives blood with antigens they do not possess, their antibodies will attack the foreign red blood cells, leading to a potentially life-threatening transfusion reaction. For example, a person with Type A blood (and anti-B antibodies) cannot receive Type B or Type AB blood because their antibodies would agglutinate (clump) the transfused red blood cells.
The Rh Factor: D Antigen and Sensitization
The Rh factor, most commonly referred to as Rh positive (Rh+) or Rh negative (Rh-), is another crucial antigen system. It’s primarily determined by the presence or absence of the D antigen on red blood cells.
- Rh Positive (Rh+): Individuals have the D antigen on their red blood cells. They do not naturally produce anti-D antibodies.
- Rh Negative (Rh-): Individuals lack the D antigen on their red blood cells. However, they can develop anti-D antibodies if exposed to Rh-positive blood. This exposure typically occurs through transfusion of Rh-positive blood or during pregnancy if an Rh-negative mother carries an Rh-positive fetus. This process of developing antibodies is called sensitization.
Once sensitized, an Rh-negative individual will have anti-D antibodies in their plasma. Subsequent exposure to Rh-positive blood will trigger a strong immune response, leading to the agglutination and destruction of the transfused red blood cells.
Rh-Negative Recipients: The Donor Pool
Given this understanding of blood group systems, we can now directly address what blood an Rh-negative person can receive. The compatibility hinges on both the ABO and Rh factors.
Receiving Rh-Positive Blood: A Complex Scenario
The crucial point for Rh-negative individuals is their potential to develop anti-D antibodies. Therefore, the general rule is that an Rh-negative person should ideally receive Rh-negative blood. However, the situation becomes more nuanced when considering the scarcity of blood and emergency situations.
If an Rh-negative individual has never been exposed to Rh-positive blood before, they can theoretically receive Rh-positive blood, as they have not yet developed anti-D antibodies. However, this is a risky practice and is generally avoided whenever possible. The reason for avoidance is the high likelihood of sensitization. The first transfusion might not cause a severe immediate reaction, but it would sensitize the recipient. A subsequent transfusion of Rh-positive blood would then lead to a severe hemolytic transfusion reaction.
The Safest Option: Rh-Negative Blood
For an Rh-negative recipient, the safest and most universally accepted transfusion is Rh-negative blood of the correct ABO type.
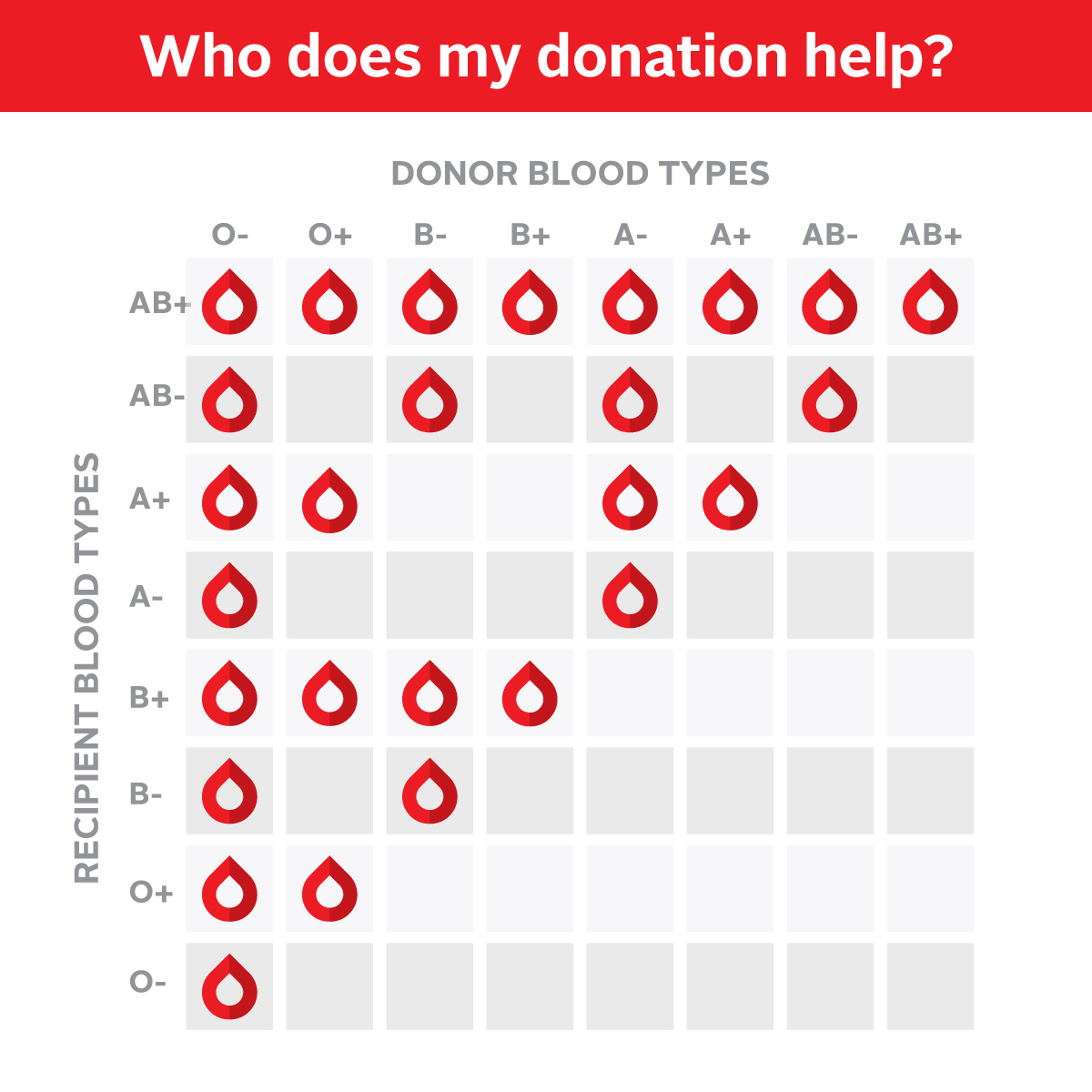
- Rh-negative Type O (O-): This blood type is often considered the universal donor for red blood cells because it lacks both A, B, and D antigens. Thus, O-negative blood can be given to virtually anyone, regardless of their ABO or Rh type, in emergencies when the recipient’s blood type is unknown.
- Rh-negative Type A (A-): Can be given to A-negative and AB-negative individuals.
- Rh-negative Type B (B-): Can be given to B-negative and AB-negative individuals.
- Rh-negative Type AB (AB-): Can be given to AB-negative individuals.
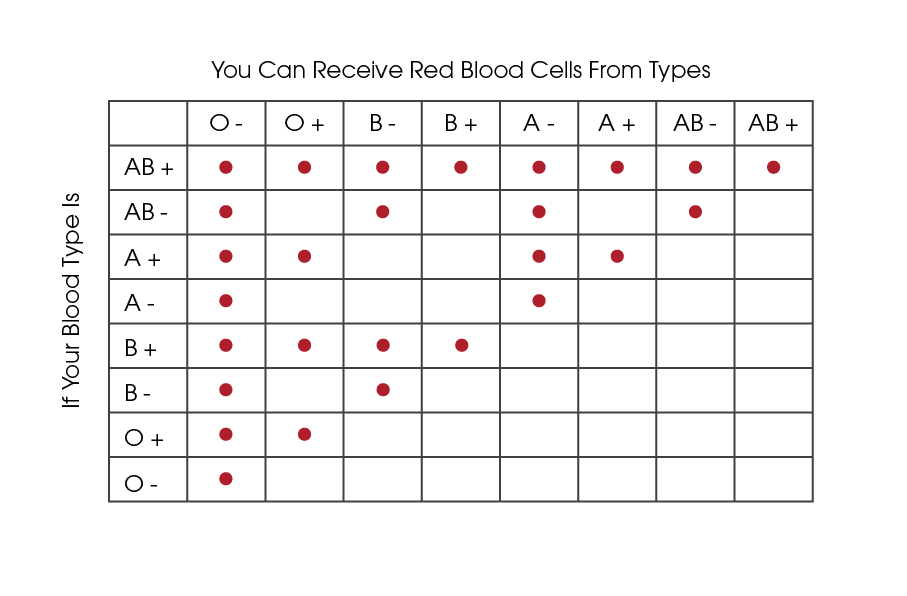
Therefore, an Rh-negative person can receive:
- Their own ABO type, Rh-negative: This is the most ideal and safest transfusion.
- Rh-negative blood from any ABO type if their own ABO type is unavailable (in emergencies): For example, an A-negative person could receive O-negative blood.
- Rh-positive blood (ABO compatible) only if absolutely necessary and they have never been previously sensitized: This is a last resort and carries significant risks of sensitization and future transfusion reactions.
The decision to administer Rh-positive blood to an Rh-negative recipient is a complex one made by medical professionals, often in critical, life-or-death situations where Rh-negative blood of the appropriate ABO type is unavailable. The risks and benefits are carefully weighed, and the patient is closely monitored.
The Criticality of Antibody Screening and Crossmatching
Beyond basic blood typing, thorough antibody screening and crossmatching are essential steps to ensure transfusion safety, particularly for individuals who may have developed antibodies to other blood group antigens besides D.
Antibody Screening: Detecting Unexpected Antibodies
When a patient’s blood is tested before a transfusion, not only is their ABO and Rh type determined, but their plasma is also screened for the presence of antibodies against other red blood cell antigens. This is known as antibody screening. It’s particularly important for patients who have:
- Previously received blood transfusions.
- Been pregnant (as pregnancy can also lead to sensitization).
- Certain medical conditions.
The presence of “unexpected antibodies” can complicate transfusions, as these antibodies can also cause transfusion reactions if the donor blood contains the corresponding antigen.
Crossmatching: Ensuring Antigen-Antibody Compatibility
Crossmatching is the final and most critical step before administering a blood transfusion. It involves mixing a sample of the recipient’s serum (plasma containing antibodies) with a sample of the donor’s red blood cells. This direct test checks for agglutination or hemolysis, confirming that there are no significant antigen-antibody reactions between the donor’s red blood cells and the recipient’s plasma.
- Major Crossmatch: Recipient’s serum + Donor’s red blood cells. This is the most crucial part, ensuring the recipient’s antibodies don’t attack the donor’s cells.
- Minor Crossmatch: Donor’s serum + Recipient’s red blood cells. This checks for antibodies in the donor’s plasma that might react with the recipient’s red blood cells. While less critical for red blood cell survival, it can be important, especially in situations with large volume transfusions.
For an Rh-negative recipient, the crossmatch will specifically ensure that the donor red blood cells are Rh-negative, and that there are no other antibodies in the recipient’s plasma that would react with antigens present on the donor red blood cells.
Implications for Rh-Negative Women and Future Pregnancies
The Rh factor has significant implications for women, particularly during pregnancy. If an Rh-negative woman carries an Rh-positive fetus, there is a risk of fetal-maternal hemorrhage, where fetal red blood cells enter the mother’s bloodstream. This can sensitize the mother, leading to the production of anti-D antibodies.
Hemolytic Disease of the Newborn (HDN)
If an Rh-negative woman who has been sensitized to the Rh factor becomes pregnant with an Rh-positive fetus again, her anti-D antibodies can cross the placenta and attack the fetus’s red blood cells. This can lead to Hemolytic Disease of the Newborn (HDN), a serious condition characterized by anemia, jaundice, and, in severe cases, hydrops fetalis (severe swelling) and fetal death.
Prevention: RhoGAM (Anti-D Immunoglobulin)
To prevent Rh sensitization and HDN, Rh-negative pregnant women are administered RhoGAM (also known as Rh immune globulin) at specific points during pregnancy and after delivery. RhoGAM contains anti-D antibodies that bind to any Rh-positive fetal red blood cells that may enter the mother’s circulation, effectively destroying them before the mother’s immune system can become sensitized. This has dramatically reduced the incidence of HDN.
Conclusion: The Importance of Precise Matching
The question of “what blood can a negative receive” underscores the vital importance of precise immunological matching in blood transfusions. For Rh-negative individuals, the primary concern is to avoid exposure to Rh-positive blood to prevent sensitization and the subsequent development of anti-D antibodies. While in dire emergencies, Rh-positive blood might be considered as a last resort for a never-sensitized Rh-negative individual, the safest and most recommended transfusion is always Rh-negative blood of the correct ABO type. Meticulous antibody screening and crossmatching remain cornerstones of transfusion medicine, ensuring the safety and efficacy of this life-saving medical intervention. The advancements in understanding blood group systems and the development of preventative measures like RhoGAM have revolutionized the management of Rh incompatibility, safeguarding both recipients and future generations.