The ability to control and coordinate the complex physiological processes involved in urination is a fundamental aspect of human health. When this intricate system falters, it can lead to a range of debilitating issues collectively known as voiding dysfunction. This umbrella term encompasses a spectrum of conditions where the bladder or the urinary tract’s ability to store and release urine is impaired, resulting in involuntary leakage, difficulty emptying, or a combination of both. Understanding voiding dysfunction is crucial for diagnosis, effective management, and improving the quality of life for millions affected worldwide.
At its core, normal voiding is a finely tuned interplay between the nervous system and the muscular components of the urinary tract. The bladder, a muscular organ, stores urine produced by the kidneys. Its walls contain smooth muscle (the detrusor muscle) that relaxes to allow filling and contracts to expel urine. Surrounding the bladder neck and urethra are sphincter muscles, which remain contracted to prevent leakage during filling. The nervous system, comprising both the central (brain and spinal cord) and peripheral (nerves connecting to the bladder and sphincters) branches, acts as the control center, sending signals to coordinate relaxation and contraction at the appropriate times. Urination, or voiding, is a voluntary process initiated by the brain when the bladder reaches a certain fullness. This involves coordinated signals that cause the detrusor muscle to contract and the sphincter muscles to relax, allowing urine to flow freely through the urethra and out of the body.
Voiding dysfunction disrupts this delicate balance, leading to a variety of symptoms that can significantly impact daily life. These symptoms can range from mild annoyance to severe incapacitation, affecting individuals of all ages and genders. Recognizing the signs and understanding the underlying mechanisms are the first steps towards addressing these challenges.
Understanding the Mechanisms of Normal Voiding
To fully grasp what goes wrong in voiding dysfunction, it is essential to first understand how the normal voiding process works. This involves a complex neuromuscular coordination that ensures efficient urine storage and controlled release.
The Role of the Bladder and Urethra
The bladder acts as a reservoir, capable of expanding significantly to accommodate urine. Its walls are primarily composed of the detrusor muscle, a type of involuntary smooth muscle. During the filling phase, the detrusor muscle remains relaxed, allowing the bladder to fill with urine without a significant increase in internal pressure. The internal urethral sphincter, located at the bladder neck, is tonically contracted, preventing urine from leaking out. The urethra is the tube that carries urine from the bladder out of the body. Its lining is also designed to prevent leakage, and the external urethral sphincter, made of voluntary skeletal muscle, provides an additional layer of control.
The Nervous System’s Control Over Voiding
The nervous system plays a pivotal role in both the storage and emptying phases of bladder function. The sacral segments of the spinal cord are central to bladder control.
- Sensory Input: As the bladder fills, stretch receptors in the bladder wall send signals via afferent nerves (sensory nerves) to the spinal cord and then to the brain. These signals inform the brain about bladder fullness.
- Parasympathetic Nervous System: When the brain decides it is appropriate to void, it sends signals down the spinal cord to the sacral nerves, which stimulate the parasympathetic nervous system. This stimulation causes the detrusor muscle to contract, increasing bladder pressure.
- Sympathetic Nervous System: During the filling phase, the sympathetic nervous system normally inhibits detrusor muscle contraction and promotes contraction of the internal urethral sphincter, aiding in urine storage.
- Somatic Nervous System: The somatic nervous system controls the external urethral sphincter. For voluntary voiding to occur, the brain sends signals that inhibit the somatic nerves supplying the external sphincter, causing it to relax.
This coordinated efferent signaling, involving both the parasympathetic and somatic pathways, ensures that the bladder empties effectively while preventing leakage at other times.
Types and Manifestations of Voiding Dysfunction
Voiding dysfunction is not a single entity but rather a broad category encompassing various conditions that disrupt the normal flow of urine. These conditions can be broadly classified based on whether the primary issue is related to the bladder’s ability to store urine or its ability to empty effectively.
Storage Problems: Overactive Bladder and Incontinence
When the bladder has difficulty storing urine, it often leads to symptoms of urinary urgency and frequency, and in many cases, urinary incontinence.
Overactive Bladder (OAB)
Overactive bladder is characterized by involuntary contractions of the detrusor muscle during the bladder filling phase. This can occur even when the bladder is not full, leading to a sudden, strong urge to urinate that is difficult to suppress.
- Urgency: The hallmark symptom of OAB, defined as a sudden, compelling desire to urinate that is difficult to defer.
- Frequency: The need to urinate more often than is considered normal (typically more than eight times in 24 hours).
- Nocturia: Waking up more than once during the night to urinate.
- Urge Incontinence: The involuntary leakage of urine that occurs immediately following or accompanying the sensation of urgency.
The causes of OAB are diverse and can include neurological conditions (such as stroke, Parkinson’s disease, or multiple sclerosis), bladder outlet obstruction (like an enlarged prostate in men), urinary tract infections, or sometimes the cause remains unknown (idiopathic OAB).
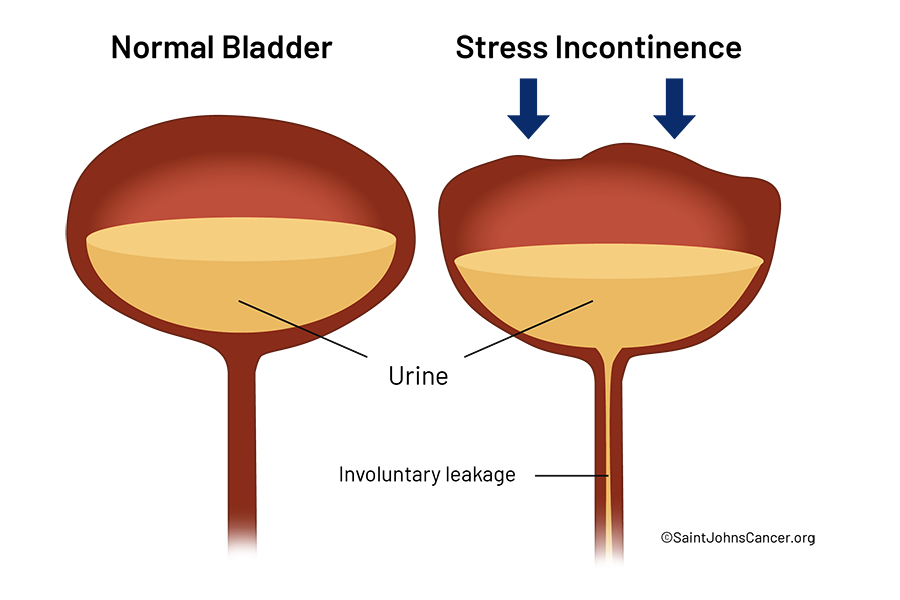
Stress Urinary Incontinence (SUI)
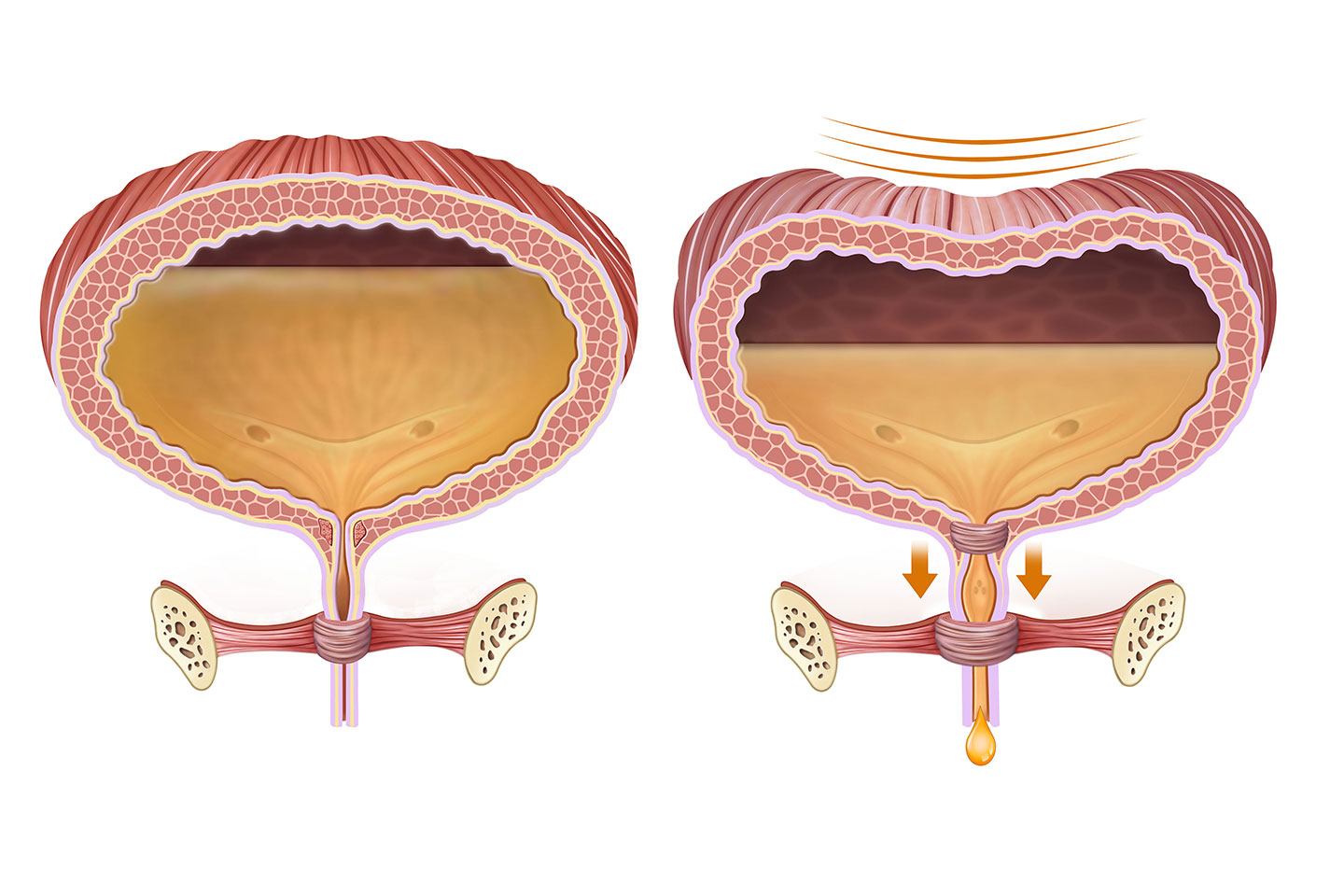
Stress urinary incontinence is the involuntary loss of urine that occurs during activities that increase intra-abdominal pressure, such as coughing, sneezing, laughing, exercising, or lifting heavy objects. This is typically due to weakness or damage to the pelvic floor muscles and/or the urinary sphincters that normally provide support and closure.
- Mechanism: In SUI, the urethral sphincter mechanism is compromised. When intra-abdominal pressure rises, it is transmitted to the bladder but not adequately to the urethra, allowing urine to escape.
- Causes: Common causes include childbirth (especially vaginal delivery), pregnancy, obesity, chronic coughing (from conditions like COPD or smoking), and aging. Surgical procedures in the pelvic region can also contribute.
Emptying Problems: Underactive Bladder and Retention
When the bladder struggles to empty effectively, it can lead to urine retention and a range of other complications.
Underactive Bladder (UAB)
Underactive bladder, also known as detrusor underactivity, is a condition where the detrusor muscle has weakened contractility, resulting in incomplete bladder emptying. This can manifest as difficulty initiating urination, a weak urine stream, and a feeling of incomplete emptying.
- Symptoms:
- Hesitancy: Difficulty starting the urine stream.
- Straining: Needing to push or strain to urinate.
- Intermittency: The urine stream starts and stops.
- Feeling of incomplete emptying: The sensation that the bladder is not empty after urinating.
- Urinary retention: The inability to empty the bladder completely.
- Causes: UAB can be caused by neurological conditions affecting the nerves that control the bladder (e.g., diabetes, spinal cord injuries, multiple sclerosis), aging, prolonged bladder outlet obstruction that has led to detrusor muscle fatigue, or certain medications.
Bladder Outlet Obstruction (BOO)
Bladder outlet obstruction occurs when there is a physical blockage in the pathway that urine travels from the bladder to the outside of the body. This obstruction forces the bladder to work harder to expel urine.
- In Men: The most common cause of BOO is benign prostatic hyperplasia (BPH), an enlargement of the prostate gland that surrounds the urethra. Other causes include prostate cancer and urethral strictures (narrowing of the urethra).
- In Women: BOO is less common but can be caused by pelvic organ prolapse (where organs like the bladder or uterus descend), urethral strictures, or tumors.
- Consequences: BOO can lead to symptoms similar to those of UAB, including hesitancy, straining, a weak stream, and incomplete emptying. Over time, the bladder muscle may eventually weaken, leading to a secondary diagnosis of detrusor underactivity.
Diagnosis and Management Strategies
Accurate diagnosis is paramount in effectively managing voiding dysfunction. A thorough medical history, physical examination, and targeted investigations are essential to identify the underlying cause and guide treatment.
Diagnostic Evaluation
The diagnostic process for voiding dysfunction typically involves several steps to comprehensively assess bladder function and identify potential contributing factors.
- Medical History and Physical Examination: A detailed review of symptoms, including their onset, severity, and impact on daily life, is crucial. The physician will also inquire about medical history, medications, and lifestyle factors. A physical examination may include a neurological assessment and, in women, a pelvic exam, and in men, a digital rectal exam to assess the prostate.
- Urinalysis and Urine Culture: These tests help to rule out urinary tract infections, which can mimic or exacerbate voiding dysfunction symptoms.
- Voiding Diary (Bladder Diary): This is a critical tool where the patient records fluid intake, voiding times, urine volume, and any episodes of leakage or urgency over a period of 2–7 days. It provides objective data on bladder habits and patterns.
- Uroflowmetry: This non-invasive test measures the speed and volume of the urine stream. It can help identify obstructions or diminished bladder contractility.
- Post-Void Residual (PVR) Measurement: Ultrasound or catheterization is used to measure the amount of urine remaining in the bladder after voiding. A high PVR indicates incomplete emptying.
- Urodynamic Studies: These are a series of tests that provide a detailed assessment of bladder function. They can include:
- Cystometry: Measures bladder pressure during filling and voiding to assess bladder capacity and detrusor muscle activity.
- Pressure-Flow Studies: Combine cystometry with uroflowmetry to analyze the relationship between bladder pressure and urine flow rate, helping to diagnose bladder outlet obstruction or detrusor underactivity.
- Sphincter Electromyography (EMG): Assesses the electrical activity of the urethral sphincter muscles, which can help identify neurological issues affecting sphincter control.
Treatment Approaches
The management of voiding dysfunction is tailored to the specific diagnosis, with treatment goals focused on improving symptoms, restoring continence, and preventing complications.
Lifestyle Modifications and Behavioral Therapies
These are often the first line of treatment and can be highly effective for many individuals.
- Fluid Management: Adjusting fluid intake, particularly reducing intake before bedtime, can help manage frequency and nocturia.
- Dietary Changes: Avoiding bladder irritants like caffeine, alcohol, and spicy foods can reduce urgency and frequency in some cases.
- Timed Voiding: Establishing a regular voiding schedule, rather than waiting for the urge to urinate, can help retrain the bladder and improve control.
- Pelvic Floor Muscle Training (Kegel Exercises): Strengthening the pelvic floor muscles can improve support for the bladder and urethra, which is particularly beneficial for stress urinary incontinence and can also help with urge incontinence.
- Bladder Retraining: This involves gradually increasing the time between voids to improve bladder capacity and reduce urgency.
Medications
Various medications can be prescribed to manage different types of voiding dysfunction.
- Anticholinergics/Antimuscarinics: These drugs (e.g., oxybutynin, tolterodine) relax the detrusor muscle and are effective in reducing bladder contractions, thus treating urgency and urge incontinence associated with OAB.
- Beta-3 Adrenergic Agonists: Mirabegron is another medication that relaxes the detrusor muscle and is an alternative to anticholinergics for OAB.
- Alpha-Blockers: In men with BPH, alpha-blockers (e.g., tamsulosin, alfuzosin) relax the smooth muscle in the prostate and bladder neck, improving urine flow and easing voiding.
- 5-Alpha Reductase Inhibitors: These medications (e.g., finasteride, dutasteride) reduce the size of the prostate gland over time, also alleviating BPH symptoms.
- Estrogen Therapy (Topical): For postmenopausal women, topical estrogen can help improve the health and elasticity of the vaginal and urethral tissues, potentially alleviating mild stress and urge incontinence.
Advanced Therapies and Surgical Interventions
When conservative and medical treatments are insufficient, more advanced options may be considered.
- Botulinum Toxin (Botox) Injections: Botulinum toxin can be injected into the detrusor muscle to temporarily paralyze it, effectively reducing involuntary contractions and treating severe OAB or neurogenic bladder.
- Nerve Stimulation:
- Sacral Neuromodulation (SNM): A small device is implanted near the sacral nerves to send electrical impulses to the bladder, regulating its function. It is used for OAB, non-obstructive urinary retention, and fecal incontinence.
- Percutaneous Tibial Nerve Stimulation (PTNS): A needle electrode is inserted near the ankle to stimulate the tibial nerve, which shares nerve pathways with the bladder. It is a less invasive option for OAB.
- Surgery: Surgical interventions are typically reserved for cases of significant anatomical issues or when other treatments have failed.
- Sling Procedures: For stress urinary incontinence in women, slings are placed to support the urethra.
- Artificial Urinary Sphincter: An artificial device implanted to control urine flow, typically used for severe SUI in men.
- Prostate Surgery: Procedures like transurethral resection of the prostate (TURP) or minimally invasive techniques are used to remove obstructing prostate tissue in men.
- Bladder Augmentation or Diversion: In severe cases of bladder dysfunction, surgery to enlarge the bladder or create a diversion for urine may be necessary.
In conclusion, voiding dysfunction is a complex group of disorders that significantly affect an individual’s well-being. By understanding the intricate mechanisms of normal voiding, recognizing the diverse manifestations of dysfunction, and employing a comprehensive diagnostic and management approach, healthcare professionals can work towards restoring bladder control and enhancing the quality of life for those affected. The journey from symptom to resolution often involves a combination of lifestyle adjustments, medical therapies, and sometimes, advanced interventions, underscoring the personalized nature of treatment for these challenging conditions.