Wegener’s granulomatosis, now more commonly known as Granulomatosis with Polyangiitis (GPA), is a rare and serious autoimmune disease. It falls under the umbrella of vasculitis, a group of disorders characterized by inflammation of blood vessels. This inflammation can affect various parts of the body, but GPA specifically targets small to medium-sized blood vessels, particularly those in the respiratory system (nose, sinuses, throat, lungs) and the kidneys. However, it can also impact the eyes, skin, ears, and nervous system. The disease’s insidious onset and wide-ranging potential manifestations can make diagnosis challenging, often leading to delays in treatment, which can have significant consequences. Understanding GPA, its pathogenesis, symptoms, and management is crucial for early detection and improved patient outcomes.
Understanding the Pathogenesis of Granulomatosis with Polyangiitis
At its core, GPA is an autoimmune condition, meaning the body’s own immune system mistakenly attacks healthy tissues. The precise trigger for this aberrant immune response remains somewhat elusive, but research points to a complex interplay of genetic predisposition, environmental factors, and an abnormal immune cell activation.
The Role of Autoantibodies
A key hallmark of GPA is the presence of specific autoantibodies in the blood. The most commonly identified are anti-neutrophil cytoplasmic antibodies (ANCAs). Neutrophils are a type of white blood cell crucial for fighting infections. In GPA, the immune system produces antibodies that target components within these neutrophils, such as proteinase 3 (PR3) and myeloperoxidase (MPO).
- Anti-PR3 Antibodies: These are found in the majority of GPA patients and are strongly associated with the disease. When antibodies bind to PR3, they can activate neutrophils.
- Anti-MPO Antibodies: While less common than anti-PR3, anti-MPO antibodies are also seen in some GPA patients and can contribute to the inflammatory process.
Neutrophil Activation and Inflammation
The presence of ANCAs, often in conjunction with other inflammatory signals, leads to the activation of neutrophils. Activated neutrophils release their destructive enzymes and reactive oxygen species, intending to combat perceived threats. However, in GPA, this process occurs inappropriately and indiscriminately, damaging the walls of blood vessels.
- Granuloma Formation: The “granulomatosis” in the older name refers to the formation of granulomas – collections of inflammatory cells, often macrophages, that attempt to wall off the inflammation. While granulomas are a characteristic feature, they are not always present or easily identifiable.
- Pauci-immune Vasculitis: GPA is classified as a pauci-immune vasculitis. This means that the inflammation in the blood vessel walls is characterized by a lack of immune complex deposition, distinguishing it from other forms of vasculitis. The damage is primarily driven by the direct attack of activated immune cells.
Consequences of Blood Vessel Inflammation
The inflammation and damage to blood vessel walls have profound consequences for the organs they supply. The compromised blood flow and tissue damage can lead to:
- Ischemia: Reduced blood supply to tissues and organs.
- Ulceration: Open sores, particularly in the respiratory tract and on the skin.
- Hemorrhage: Bleeding due to damaged vessel walls.
- Organ Dysfunction: Impaired function of affected organs like the lungs and kidneys.
The specific pattern of organ involvement is highly variable among individuals with GPA, contributing to the diverse clinical presentations of the disease.
Clinical Manifestations: A Diverse and Evolving Picture
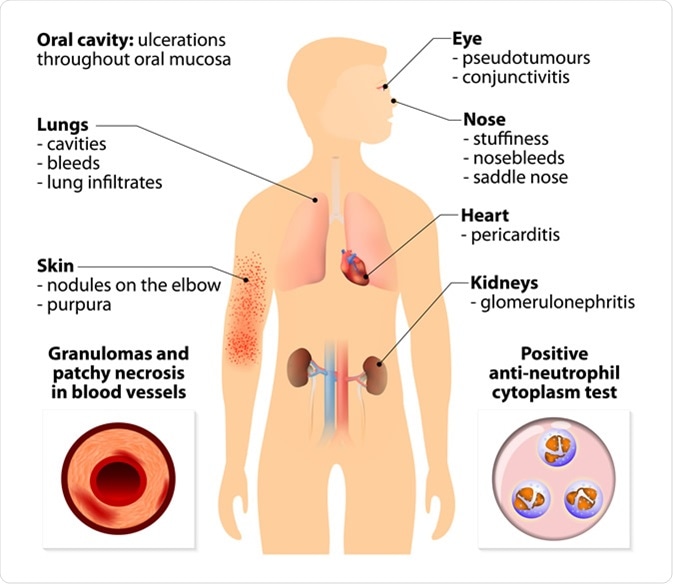
The symptoms of GPA can vary widely depending on which organs are affected and the severity of the inflammation. The onset can be gradual, with non-specific symptoms, or acute and severe. Often, patients present with a combination of upper and lower respiratory tract symptoms, along with evidence of kidney involvement.
Upper Respiratory Tract Involvement
The nasal passages, sinuses, and throat are frequently the initial sites of inflammation. Symptoms can include:
- Persistent Sinusitis: Chronic sinus inflammation that doesn’t respond to typical treatments.
- Nasal Symptoms: Runny nose, crusting, nosebleeds (epistaxis), and a saddle nose deformity due to cartilage destruction.
- Sore Throat and Ear Infections: Inflammation can extend to the throat and middle ear, causing pain and hearing loss.
- Laryngeal Involvement: In rarer cases, inflammation can affect the larynx, leading to hoarseness or difficulty breathing.
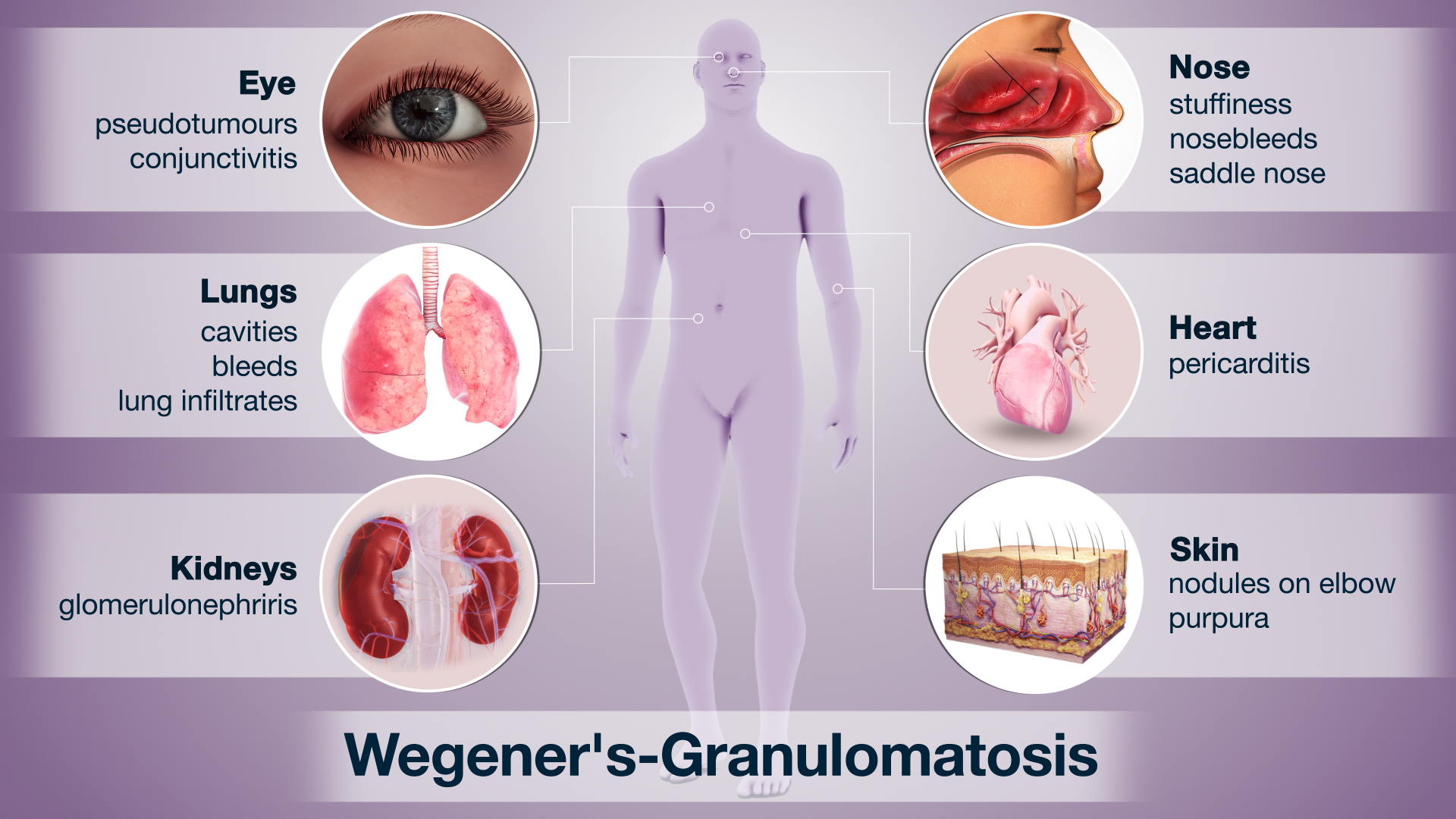
Lower Respiratory Tract Involvement
The lungs are another common site for GPA, leading to a range of respiratory symptoms:
- Cough: Often dry and persistent, but can produce blood-tinged sputum (hemoptysis).
- Shortness of Breath (Dyspnea): Resulting from inflammation and scarring in the lung tissue.
- Chest Pain: Especially with deep breaths.
- Lung Nodules and Cavities: X-rays and CT scans often reveal characteristic lesions in the lungs, which can be nodules, infiltrates, or cavities.
Kidney Involvement (Renal Vasculitis)
Kidney involvement is a critical and potentially life-threatening manifestation of GPA. The inflammation damages the small blood vessels (glomeruli) in the kidneys, impairing their ability to filter waste products from the blood.
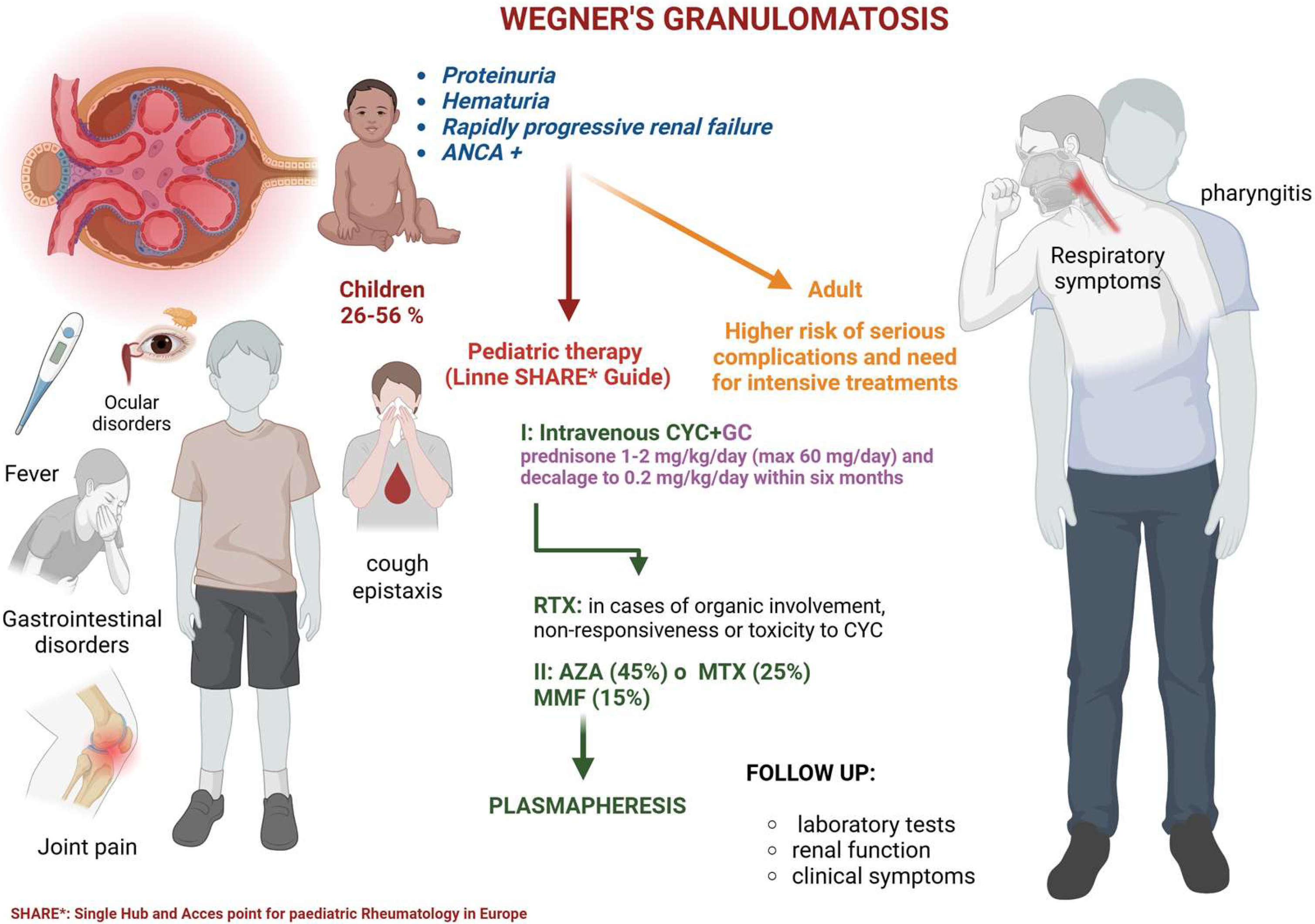
- Hematuria: Blood in the urine, often microscopic but sometimes visible.
- Proteinuria: Excess protein in the urine.
- Kidney Failure: In severe cases, GPA can rapidly lead to end-stage renal disease, requiring dialysis or a kidney transplant.
- Hypertension: High blood pressure is a common consequence of kidney damage.
Other Systemic Manifestations
Beyond the respiratory system and kidneys, GPA can affect numerous other organs and systems:
- Ocular Involvement: Inflammation of the eyes can manifest as redness, pain, blurred vision, and even vision loss. This can involve the orbit, conjunctiva, sclera, and uvea.
- Cutaneous Manifestations: Skin lesions are common and can include purpura (bruises), ulcers, nodules, and livedo reticularis (a mottled, lace-like pattern of discoloration).
- Neurological Involvement: Peripheral neuropathy (nerve damage in the limbs) causing numbness, tingling, or weakness is a significant concern. Central nervous system involvement, though less common, can lead to headaches, seizures, or strokes.
- Musculoskeletal Symptoms: Joint pain (arthralgia) and inflammation (arthritis) are frequent.
- Constitutional Symptoms: General symptoms such as fever, fatigue, weight loss, and night sweats are often present, particularly during active disease flares.
Diagnosis and Management of Granulomatosis with Polyangiitis
Diagnosing GPA requires a comprehensive approach that integrates clinical findings, laboratory tests, and often tissue biopsy. Once diagnosed, treatment aims to suppress the overactive immune system and prevent further organ damage.
Diagnostic Evaluation
The diagnostic process for GPA typically involves:
- Medical History and Physical Examination: A thorough review of symptoms and a physical assessment looking for signs of vasculitis in various organ systems.
- Blood Tests:
- ANCA Testing: Detection of anti-PR3 or anti-MPO antibodies is crucial, although a positive ANCA alone is not diagnostic.
- Inflammatory Markers: Elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) indicate inflammation.
- Kidney Function Tests: Blood urea nitrogen (BUN) and creatinine levels to assess kidney function.
- Urinalysis: To detect blood and protein in the urine.
- Imaging Studies:
- Chest X-ray and CT Scan: To identify lung lesions, nodules, or infiltrates.
- Sinus CT Scan: To assess inflammation in the paranasal sinuses.
- Biopsy: A tissue biopsy from an affected organ (e.g., kidney, lung, skin, nasal mucosa) is often considered the gold standard for confirming the diagnosis. The biopsy will reveal characteristic inflammatory changes, including vasculitis and, sometimes, granuloma formation.
Treatment Strategies
The management of GPA is multifaceted and typically involves a combination of medications. The goal is to achieve remission (symptom-free state) and then maintain it while minimizing treatment-related side effects.
- Induction of Remission: This initial phase focuses on aggressively controlling the disease.
- Corticosteroids: High-dose glucocorticoids (e.g., prednisone) are the cornerstone of treatment to rapidly reduce inflammation.
- Immunosuppressive Agents: In addition to corticosteroids, more potent immunosuppressants are used to achieve and maintain remission. Common agents include:
- Cyclophosphamide: A powerful cytotoxic drug that was historically a mainstay for induction, particularly in severe cases. However, due to its significant side effects, its use is becoming more targeted.
- Rituximab: A monoclonal antibody that targets B cells, which play a crucial role in producing ANCAs. Rituximab has emerged as a highly effective and often preferred option for both induction and maintenance of remission, with a potentially better safety profile than cyclophosphamide.
- Methotrexate: May be used for less severe disease or as a steroid-sparing agent.
- Maintenance of Remission: Once remission is achieved, treatment is gradually tapered but often continued for an extended period (typically 12-24 months or longer) to prevent relapse.
- Lower doses of corticosteroids and less toxic immunosuppressants like methotrexate or rituximab are commonly used for maintenance.
- Supportive Care: Management also includes addressing specific organ damage and symptoms:
- Blood Pressure Control: Medications to manage hypertension.
- Kidney Support: Management of kidney disease, including dialysis if necessary.
- Pain Management: For joint pain or other discomfort.
- Infection Prophylaxis: Due to immunosuppression, patients are at increased risk of infections.
Monitoring and Prognosis
Regular monitoring for disease activity and treatment side effects is essential. This involves periodic clinical assessments, blood tests (ANCA levels, inflammatory markers, kidney function), and urine tests.
The prognosis for GPA has significantly improved with advances in treatment. While it remains a serious chronic disease, many patients can achieve long-term remission and maintain a good quality of life. However, relapses can occur, and long-term complications, such as kidney damage, lung scarring, and increased risk of infections, need to be managed. Early diagnosis and prompt, aggressive treatment are paramount to achieving the best possible outcomes for individuals living with Granulomatosis with Polyangiitis.