Fibrotic tissue, often referred to as scarring, is a fundamental component of the body’s healing process. When tissues are injured, whether by trauma, inflammation, or disease, the body initiates a complex repair mechanism. A key element of this mechanism is the deposition of extracellular matrix (ECM), primarily collagen, by specialized cells called fibroblasts. While this process is essential for restoring tissue integrity and preventing further damage, excessive or aberrant fibrotic tissue formation can lead to significant organ dysfunction and disease. Understanding the nature, formation, and implications of fibrotic tissue is crucial for both medical professionals and individuals seeking to comprehend various health conditions.
The Cellular and Molecular Basis of Fibrosis
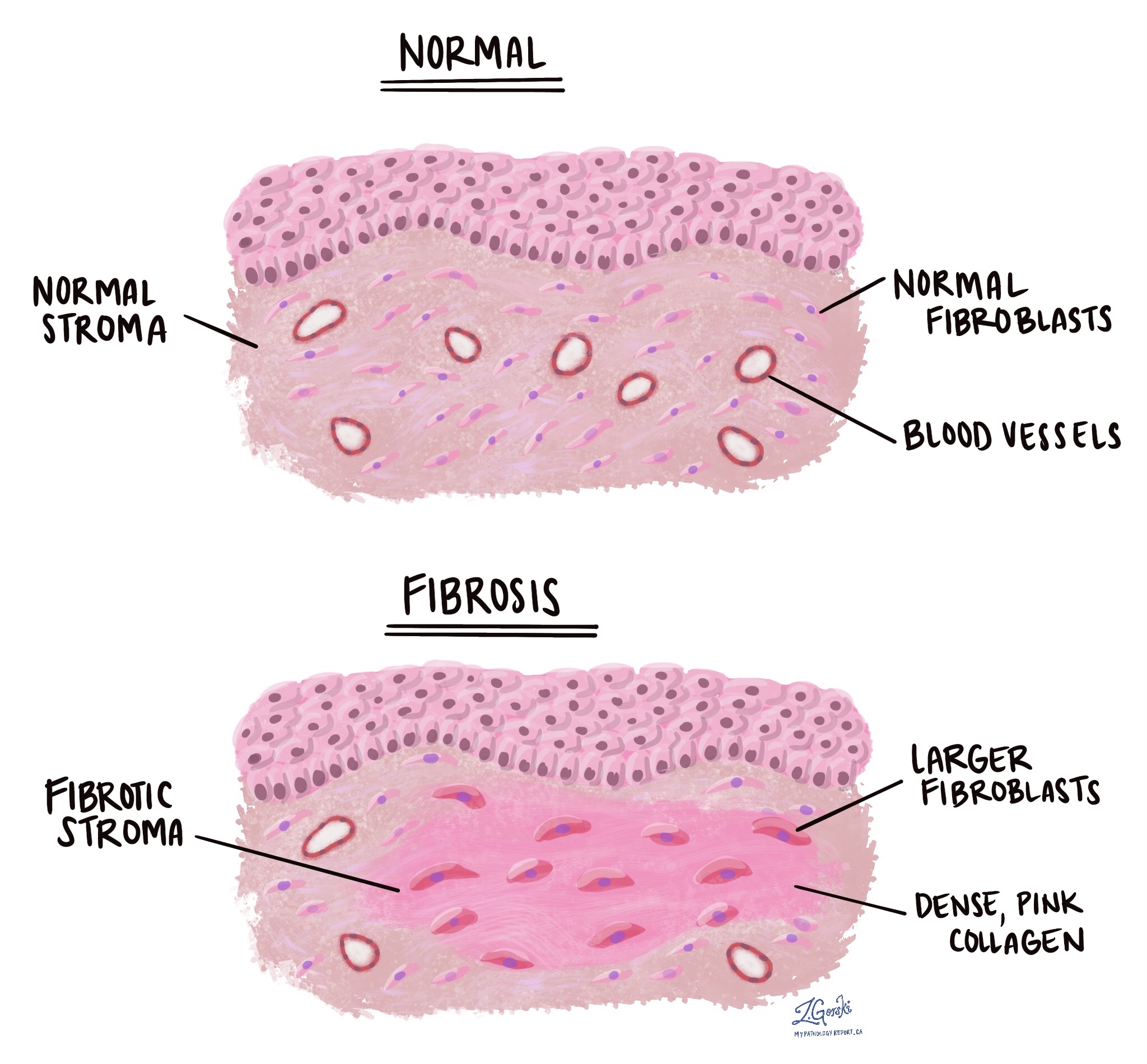
Fibrosis is not a static condition but rather a dynamic and intricate biological process involving a cascade of cellular and molecular events. At its core, fibrosis is characterized by the excessive accumulation of ECM proteins, predominantly collagen. This process is initiated and perpetuated by a complex interplay between various cell types and signaling molecules, transforming a healthy tissue into one that is stiff, scarred, and impaired in its function.
Fibroblasts: The Architects of Scarring
Fibroblasts are the primary effector cells responsible for the synthesis and deposition of ECM components, including collagen. In healthy tissues, fibroblasts exist in a quiescent state, playing a role in maintaining the structural integrity of the ECM. However, upon injury or chronic inflammation, these cells undergo a remarkable transformation. They become activated, transitioning into myofibroblasts. Myofibroblasts are characterized by their enhanced migratory capacity, increased proliferation, and significantly upregulated production of ECM proteins. This activation is often triggered by growth factors and cytokines released by damaged cells and inflammatory cells.
Activation Pathways of Fibroblasts
The activation of fibroblasts into myofibroblasts is a tightly regulated process, though it can become dysregulated in fibrotic diseases. A key signaling pathway involves the transforming growth factor-beta (TGF-β) superfamily. TGF-β is a potent pro-fibrotic cytokine that binds to specific receptors on fibroblasts, initiating intracellular signaling cascades. These cascades lead to the expression of genes responsible for collagen synthesis, myofibroblast differentiation, and the production of other ECM components like fibronectin and proteoglycans.
Another critical player in fibroblast activation is platelet-derived growth factor (PDGF). PDGF can stimulate fibroblast proliferation and migration, further contributing to the accumulation of these cells at the injury site. Additionally, cytokines such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α), which are hallmarks of inflammation, can also promote fibroblast activation and the fibrotic process.
Extracellular Matrix Deposition and Remodeling
The hallmark of fibrotic tissue is the excessive deposition of ECM proteins. While ECM is a normal and vital component of all tissues, providing structural support and regulating cell behavior, its excessive accumulation in fibrosis leads to detrimental consequences. Collagen, particularly types I and III, is the most abundant protein in fibrotic scars. Its deposition occurs in a disorganized manner, forming dense, avascular scar tissue that replaces functional tissue.
Components of the Extracellular Matrix in Fibrosis
Beyond collagen, other ECM components are also altered in fibrotic tissue. Fibronectin, a glycoprotein involved in cell adhesion and migration, is often overexpressed. Hyaluronic acid, a glycosaminoglycan that contributes to tissue hydration and lubrication, can also be modified in its quantity and structure. The balance between ECM synthesis and degradation is crucial for normal tissue homeostasis. In fibrosis, this balance is disrupted, with synthesis significantly outweighing degradation. Enzymes responsible for ECM degradation, known as matrix metalloproteinases (MMPs), are often downregulated or inhibited by their natural inhibitors, further contributing to ECM accumulation.
The Role of Inflammation
Inflammation is often a trigger and a perpetuating factor for fibrosis. During an initial injury, inflammatory cells such as macrophages are recruited to the site. These cells, while initially important for clearing debris and initiating repair, can also release pro-fibrotic mediators. For example, macrophages can secrete TGF-β and other cytokines that stimulate fibroblast activation. Chronic inflammation, characterized by the sustained presence of inflammatory cells and the continuous release of inflammatory mediators, can create a persistent pro-fibrotic microenvironment, driving ongoing ECM deposition and scar formation. This is particularly evident in conditions like chronic hepatitis, where ongoing viral infection or autoimmune attack leads to persistent liver inflammation and subsequent fibrosis.
Pathological Manifestations and Organ-Specific Fibrosis
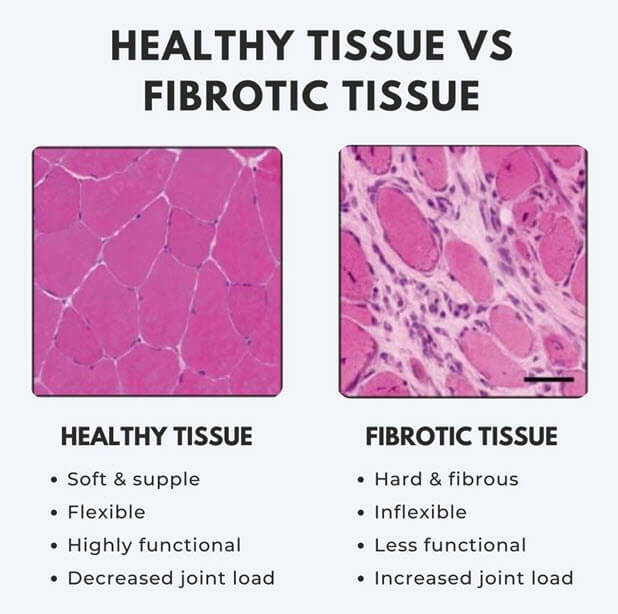
Fibrotic tissue, by its nature of replacing functional tissue with scar material, can impair the ability of organs to perform their essential tasks. The consequences of fibrosis are highly organ-specific, leading to a wide spectrum of diseases. The degree of functional impairment depends on the extent of fibrosis and the specific organ affected.
Lungs and Pulmonary Fibrosis
In the lungs, excessive fibrotic tissue deposition leads to pulmonary fibrosis. This condition is characterized by the stiffening of lung tissue, making it difficult for the lungs to expand and contract effectively. This reduces the surface area available for gas exchange, leading to shortness of breath, particularly during exertion. Conditions like idiopathic pulmonary fibrosis (IPF), asbestosis, and sarcoidosis are examples of lung diseases where fibrotic scarring is a prominent feature. The distorted architecture of the lungs can also lead to a predisposition to infections and other complications.
Liver and Hepatic Fibrosis
The liver is another organ highly susceptible to fibrosis. Hepatic fibrosis is often a consequence of chronic liver injury from various causes, including viral hepatitis (Hepatitis B and C), alcohol abuse, non-alcoholic fatty liver disease (NAFLD), and autoimmune diseases. In the liver, fibrotic tissue builds up in the spaces between hepatocytes, the functional cells of the liver. As fibrosis progresses, it can disrupt the normal blood flow through the liver, leading to portal hypertension. This can cause serious complications such as ascites (fluid accumulation in the abdomen), varices (enlarged veins in the esophagus), and hepatic encephalopathy (brain dysfunction due to liver failure). Advanced hepatic fibrosis leads to cirrhosis, a condition where the liver is extensively scarred and its function is severely compromised.
Heart and Cardiac Fibrosis
Cardiac fibrosis occurs when healthy heart muscle tissue is replaced by fibrotic scar tissue. This can happen following a heart attack (myocardial infarction), due to chronic conditions like hypertension or valvular heart disease, or as a result of certain genetic disorders. Fibrotic tissue in the heart is stiffer and less electrically conductive than healthy heart muscle. This can lead to impaired heart contractility, arrhythmias (irregular heartbeats), and ultimately, heart failure. The heart may struggle to pump blood effectively, leading to symptoms like fatigue, shortness of breath, and swelling in the legs and ankles.
Kidneys and Renal Fibrosis
Renal fibrosis is a common endpoint for many chronic kidney diseases. It involves the accumulation of ECM in the glomeruli (the filtering units of the kidney) and the interstitial space (the tissue surrounding the tubules). This scarring impairs the kidneys’ ability to filter waste products from the blood, leading to a decline in kidney function. Causes of renal fibrosis include diabetes (diabetic nephropathy), high blood pressure (hypertensive nephrosclerosis), glomerulonephritis, and polycystic kidney disease. As renal fibrosis progresses, it can lead to chronic kidney disease (CKD) and eventually kidney failure, requiring dialysis or a kidney transplant.
Diagnosis, Treatment, and Future Directions
Diagnosing fibrotic tissue formation often involves a combination of clinical assessment, imaging techniques, and tissue biopsy. Treatment strategies aim to halt or slow the progression of fibrosis, manage underlying causes, and mitigate the resulting organ dysfunction. However, effectively reversing established fibrosis remains a significant challenge.
Diagnostic Approaches
Clinical suspicion of fibrosis often arises from a patient’s symptoms and medical history. For example, progressive shortness of breath might suggest pulmonary fibrosis, while jaundice and abdominal swelling could point towards liver cirrhosis.
- Imaging Techniques: Various imaging modalities play a crucial role. Ultrasound can detect changes in organ texture indicative of fibrosis, particularly in the liver. Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) scans can provide more detailed anatomical information and assess the extent of scarring in organs like the lungs and heart. Specialized MRI techniques, such as diffusion-weighted imaging (DWI) and T1 mapping, are increasingly used to non-invasively quantify liver fibrosis.
- Blood Tests: Certain blood markers can indicate organ damage and inflammation, which are often precursors to fibrosis. For instance, liver function tests are crucial for assessing liver health.
- Tissue Biopsy: Histological examination of a tissue biopsy remains the gold standard for diagnosing and staging fibrosis. A small sample of the affected organ is surgically removed and examined under a microscope by a pathologist. Special stains, such as Masson’s trichrome or picrosirius red, are used to highlight collagen deposits, allowing for precise assessment of the amount and distribution of fibrotic tissue.
Therapeutic Strategies
Current therapeutic approaches for fibrosis primarily focus on addressing the underlying cause and reducing inflammation.
- Treating the Underlying Cause: If fibrosis is driven by an infection, treating the infection (e.g., with antivirals for hepatitis C) can halt further progression. Similarly, managing conditions like diabetes, hypertension, and autoimmune disorders is critical in preventing or slowing fibrotic damage.
- Anti-inflammatory Medications: Corticosteroids and other immunosuppressive drugs are used to dampen chronic inflammation, which can, in turn, reduce pro-fibrotic signaling.
- Antifibrotic Drugs: While a limited number of drugs are specifically approved for certain fibrotic conditions (e.g., pirfenidone and nintedanib for IPF), developing broadly effective antifibrotic therapies has been a significant challenge. These drugs often target specific pathways involved in fibroblast activation or ECM synthesis.

Research and Future Hope
The scientific community is actively researching new therapeutic avenues for fibrotic diseases.
- Targeting Specific Signaling Pathways: Understanding the intricate molecular pathways that drive fibrosis is paving the way for targeted therapies. Inhibitors of TGF-β, PDGF, and other pro-fibrotic mediators are under investigation.
- Cell-Based Therapies: Stem cell therapies, particularly those involving mesenchymal stem cells, are being explored for their potential to modulate the inflammatory response and promote tissue regeneration.
- Gene Therapy and Epigenetic Modulation: Emerging approaches aim to modify gene expression or epigenetic patterns that contribute to fibrotic processes.
- Early Detection and Prevention: Greater emphasis is being placed on early detection of fibrotic changes through improved diagnostic tools and preventative strategies to intercept the disease process before significant irreversible damage occurs.
In conclusion, fibrotic tissue represents a complex biological response that, while essential for healing, can lead to devastating organ damage when dysregulated. Continued research into the cellular and molecular mechanisms of fibrosis holds the promise of developing more effective diagnostic and therapeutic interventions, offering hope for millions affected by fibrotic diseases worldwide.