The realm of modern technology, particularly as it intersects with medicine and healthcare, is constantly evolving. Among the many intricate systems and terminologies that define this landscape, the concept of “E and M codes” stands out as a fundamental element for billing and reimbursement. While seemingly obscure to the uninitiated, these codes are the backbone of how healthcare providers document and are compensated for the patient evaluation and management services they render. Understanding what an E and M code is, and how it functions, is crucial for anyone involved in healthcare administration, medical billing, or even as a patient seeking clarity on their medical bills.
Understanding the Foundation of E and M Codes
At its core, an E and M code is a standardized alphanumeric identifier used by healthcare providers to describe the complexity and resource intensity of a patient encounter. These codes are published and maintained by the Centers for Medicare & Medicaid Services (CMS) and are part of the Current Procedural Terminology (CPT) code set developed by the American Medical Association (AMA). The primary purpose of E and M codes is to ensure accurate and consistent reporting of patient visits, facilitating fair reimbursement from payers, including government programs like Medicare and Medicaid, as well as private insurance companies.
The Evolution and Purpose of E and M Coding
The evolution of E and M coding reflects a continuous effort to capture the nuances of patient care. Initially, these codes were heavily weighted on objective documentation such as the number of elements examined in a physical exam and the quantity of history taken. However, as healthcare delivery became more sophisticated and focused on patient-centered care, the emphasis shifted towards the cognitive effort and medical decision-making involved in managing a patient’s health. This shift is particularly evident in the significant revisions made to E and M coding guidelines in recent years, aiming to simplify the process and better reflect the actual work performed by physicians and other qualified healthcare professionals.
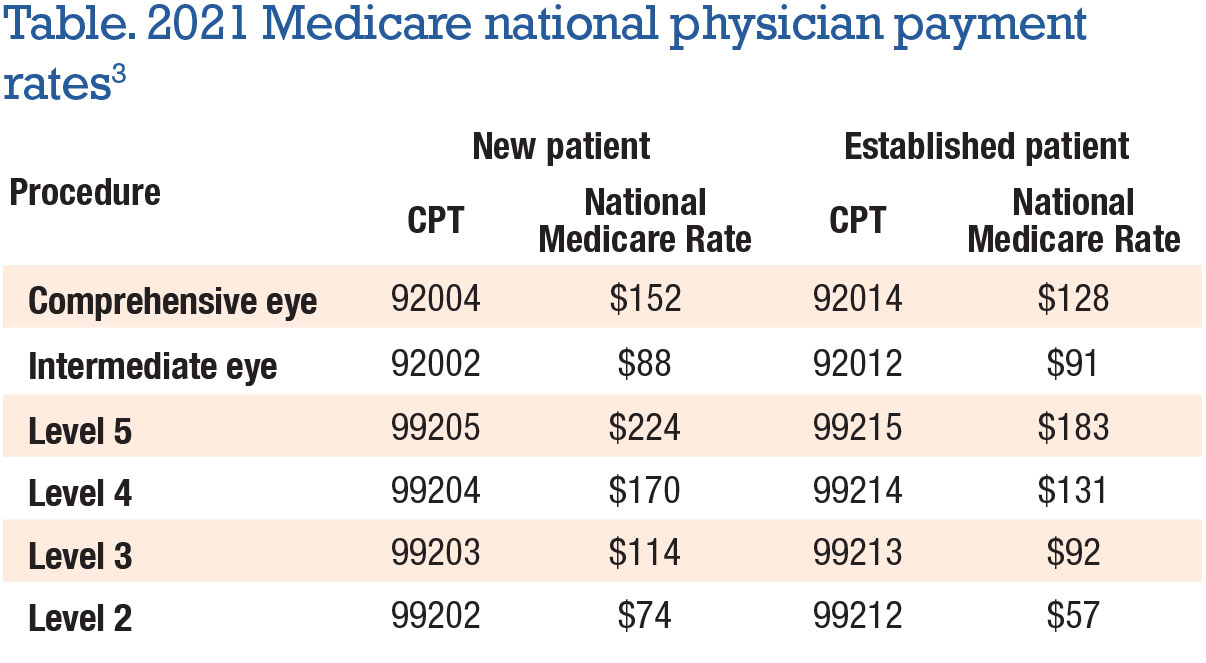
The fundamental purpose of E and M codes is multifaceted. Firstly, they provide a universal language for describing patient encounters, ensuring that all parties involved in the healthcare transaction – providers, payers, and regulatory bodies – understand the nature and scope of the services rendered. Secondly, they serve as the basis for reimbursement. Payers use these codes to determine the appropriate payment for a physician’s time and expertise. Without a standardized coding system, it would be nearly impossible to process claims efficiently and equitably. Thirdly, E and M codes contribute to data collection and analysis, offering valuable insights into healthcare utilization patterns, disease prevalence, and the effectiveness of various treatments. This data is essential for research, policy development, and public health initiatives.
Key Components of an E and M Encounter
To properly assign an E and M code, healthcare providers must meticulously document several key components of the patient encounter. These components, while subject to specific guidelines based on the type of service (e.g., office visit, hospital inpatient, emergency department), generally fall into three main categories:
History
This refers to the information gathered from the patient about their present illness, past medical history, family history, and social history. The level of detail required in the history depends on the complexity of the patient’s presentation and the chosen coding level. It aims to understand the patient’s background and the factors contributing to their current condition.
Examination
This component involves the physician’s or qualified healthcare professional’s physical assessment of the patient. The extent and nature of the examination are tailored to the patient’s presenting problem. While historically a significant driver of coding, recent changes have de-emphasized the sheer number of organ systems examined, focusing instead on the “medical necessity” and relevance of the examination to the patient’s condition.
Medical Decision Making (MDM)
This is arguably the most critical and complex component of E and M coding. MDM encompasses the thought process and judgment involved in evaluating the patient’s condition, ordering tests, interpreting results, making diagnoses, and developing a treatment plan. It considers the number and complexity of problems addressed, the amount and complexity of data to be reviewed and analyzed, and the risk of complications or death associated with the patient management or the condition of the patient. Recent revisions have placed a much greater emphasis on MDM, moving away from solely counting elements to a more nuanced assessment of the cognitive work involved.
Navigating the Levels of E and M Codes
E and M codes are structured in a hierarchical manner, with different levels representing increasing complexity and resource utilization. This tiered system allows for precise differentiation of the services provided, ensuring that providers are reimbursed appropriately for the work they undertake. The specific levels and their associated criteria have undergone significant updates, particularly for outpatient services, to better reflect the modern practice of medicine.
Outpatient Services E and M Levels
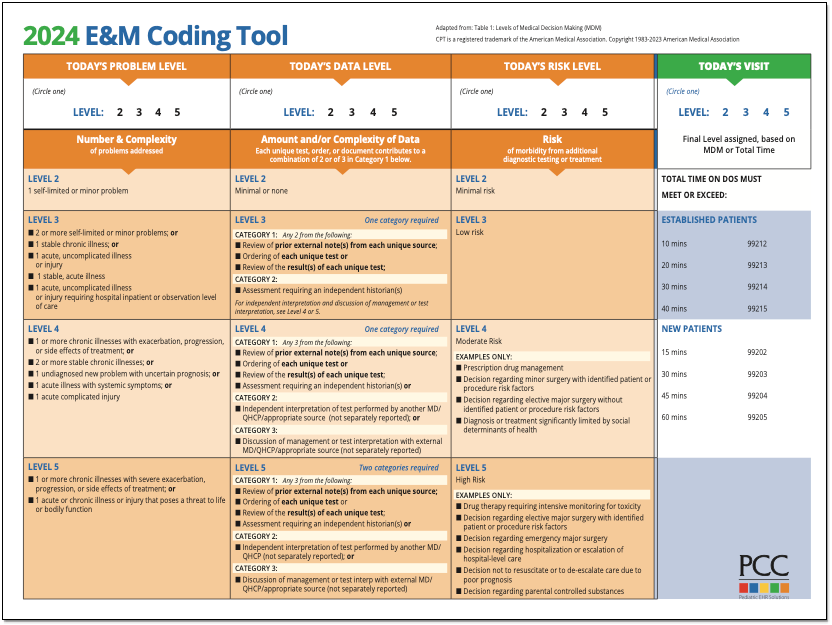
For outpatient services, such as those provided in a physician’s office or clinic, E and M codes are typically categorized by the level of service. Previously, these levels were identified by numbers (e.g., E/M Level 1, E/M Level 2, up to E/M Level 5). However, under the revised guidelines, the focus has shifted to describing the complexity of the Medical Decision Making (MDM) required. The current levels for office and other outpatient services are often described by the extent of MDM:

- Straightforward: This level involves minimal complexity in terms of problems addressed, data to be reviewed, and risk. The physician’s decision-making is typically simple and involves limited choices.
- Low Complexity: At this level, there are a limited number of self-limited or minor problems, or one stable chronic illness, or one acute, uncomplicated illness, or minor injury. The amount and complexity of data to be reviewed is minimal, and the risk is low.
- Moderate Complexity: This level involves a moderate number of self-limited or minor problems, or two or more stable chronic illnesses, or one or more undiagnosed new problems with uncertain prognosis, or one acute illness with uncertain prognosis, or significant symptom, or established illness that may not be responding to treatment. The amount and complexity of data to be reviewed is moderate, and the risk is moderate.
- High Complexity: This involves a single high-risk problem, or a moderate number of chronic illnesses all with current exacerbation, or an acute or chronic illness or injury that poses a threat to life or bodily function. The amount and complexity of data to be reviewed is extensive, and the risk is high.
The selection of the appropriate E/M code for an outpatient encounter is determined by assessing the three key components: History, Examination, and Medical Decision Making (MDM). For a significant portion of outpatient encounters, the selection of the E/M code can be based solely on the level of MDM. However, if a provider chooses to document and bill based on time, they can do so by documenting the total time spent by the physician or qualified healthcare professional on the day of the encounter and the nature of the work performed during that time.
Inpatient and Other Facility E and M Levels
Beyond outpatient settings, E and M coding also applies to services provided in other healthcare facilities, such as hospitals (inpatient, observation), emergency departments, nursing facilities, and domiciliary care. The coding structures and specific documentation requirements for these settings differ from outpatient services.
- Inpatient Services: For initial and subsequent hospital inpatient care, E/M codes reflect the physician’s work in managing a patient admitted to the hospital. The complexity is assessed based on the patient’s presenting problem, the diagnostic workup, management options, and the overall risk to the patient. Similar to outpatient services, the key components of history, examination, and medical decision making are evaluated, with a focus on the cognitive effort and resource utilization.
- Emergency Department Services: These codes are used for patients presenting to the emergency department. The coding is based on the severity of the presenting illness or injury, the extent of the workup and management, and the risk associated with the patient’s condition. Unlike other E/M services, the “time” component is generally not the primary driver for ED coding.
- Observation Services: These codes are used when a patient is admitted to a hospital for observation rather than for acute inpatient care. The coding reflects the physician’s services in managing the patient during this observation period.
- Nursing Facility Services: For residents of nursing facilities, E/M codes are used to document and bill for physician services. These codes consider the patient’s overall health status, the complexity of their medical conditions, and the services provided to manage their care within the facility.
Each of these service categories has its own set of defined E/M levels, typically ranging from 1 to 5, and specific documentation guidelines that must be followed for accurate coding and reimbursement.
The Importance of Accurate E and M Coding
In the complex landscape of healthcare reimbursement, accurate E and M coding is not merely a bureaucratic task; it is a critical component of financial stability for healthcare providers and a vital element in ensuring the integrity of the healthcare system. Errors or inconsistencies in coding can lead to a cascade of negative consequences.
Impact on Reimbursement and Revenue Cycle
The most direct impact of accurate E and M coding is on reimbursement. Payers use the assigned codes to determine the amount they will reimburse the provider for services rendered. If a provider undercodes (assigns a lower-level code than is justified by the documentation), they will be reimbursed less than the value of the services provided, negatively impacting their revenue cycle. Conversely, overcoding (assigning a higher-level code than is supported by documentation) can lead to audits, claim denials, recoupments, and even penalties for fraud. Therefore, meticulously documenting each patient encounter to support the chosen E/M code is paramount for optimizing revenue while remaining compliant.
Compliance and Auditing Considerations
The healthcare industry is heavily regulated, and accurate coding is a cornerstone of compliance. Regulatory bodies like CMS and private payers conduct regular audits to ensure that providers are adhering to coding guidelines and accurately representing the services they provide. A well-documented encounter that supports the assigned E/M code provides a strong defense against audit findings. Conversely, poor documentation or inconsistent coding practices can flag a provider for intense scrutiny, leading to significant financial penalties and reputational damage. Staying abreast of the constantly evolving E/M coding guidelines and ensuring that all staff involved in documentation and coding are properly trained is essential for mitigating compliance risks.
Data Integrity and Healthcare Analytics
Beyond direct financial implications, accurate E and M coding is fundamental to the integrity of healthcare data. The vast amounts of data generated through medical billing and coding are used for various analytical purposes, including:
- Public Health Surveillance: Tracking disease prevalence, identifying outbreaks, and monitoring public health trends.
- Quality Improvement: Measuring the quality of care delivered, identifying areas for improvement, and benchmarking performance.
- Research and Development: Supporting clinical research, developing new treatments, and understanding the effectiveness of different medical interventions.
- Resource Allocation: Informing policy decisions related to healthcare resource allocation and funding.
If the underlying E/M codes are inaccurate or inconsistent, the resulting data will be flawed, leading to misinformed decisions and potentially detrimental outcomes for public health and healthcare policy. Therefore, the commitment to accurate E/M coding extends beyond individual patient encounters to contributing to a more robust and insightful healthcare data landscape.