The human heart is a marvel of biological engineering, a tireless pump that sustains life by circulating blood throughout our bodies. Central to its function is the concept of ejection fraction (EF), a vital metric that quantifies how effectively the left ventricle, the heart’s primary pumping chamber, expels blood with each contraction. Understanding what constitutes a “normal” ejection fraction is crucial for assessing cardiovascular health and diagnosing potential heart conditions.
Understanding Ejection Fraction
Ejection fraction is not simply the amount of blood pumped, but rather the percentage of blood that is ejected from the left ventricle during one complete heartbeat. This percentage provides a snapshot of the ventricle’s contractile strength and its overall ability to meet the body’s circulatory demands.

The Mechanics of Cardiac Ejection
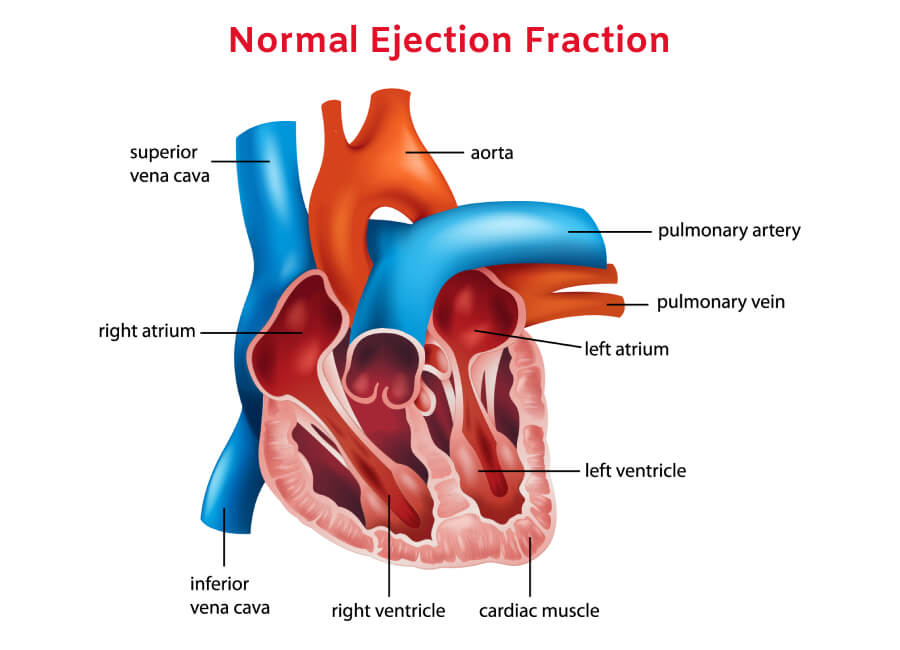
The cardiac cycle involves two main phases: diastole and systole. During diastole, the heart muscle relaxes, allowing the ventricles to fill with blood. Systole is the contraction phase, where the ventricles squeeze, pushing blood out into the pulmonary artery (from the right ventricle) and the aorta (from the left ventricle). Ejection fraction specifically measures the output from the left ventricle, as this is the chamber responsible for pumping oxygenated blood to the rest of the body.
Calculating Ejection Fraction
Ejection fraction is typically calculated using the following formula:
EF = (End-Diastolic Volume – End-Systolic Volume) / End-Diastolic Volume * 100%
- End-Diastolic Volume (EDV): This represents the total volume of blood in the left ventricle at the end of diastole, just before it contracts. It’s the maximum volume the ventricle holds.
- End-Systolic Volume (ESV): This is the volume of blood remaining in the left ventricle after it has contracted (systole).
The difference between EDV and ESV is the stroke volume – the amount of blood ejected with each beat. By dividing the stroke volume by the EDV and multiplying by 100, we arrive at the percentage that defines the ejection fraction.
Diagnostic Tools for Measuring EF
Several non-invasive imaging techniques are used to measure ejection fraction. Echocardiography, often referred to as an “echo,” is the most common. This ultrasound of the heart provides real-time images and allows for precise measurement of ventricular volumes. Other methods include cardiac magnetic resonance imaging (MRI) and cardiac computed tomography (CT) scans, which can offer more detailed anatomical information and, in some cases, more accurate EF calculations. Nuclear cardiology tests can also be employed.
What is Considered a Normal Ejection Fraction?
The definition of a “normal” ejection fraction is generally consistent across medical guidelines, though slight variations can exist due to factors like age, sex, and the specific diagnostic method used. However, a clear range is established for healthy cardiac function.
The Standard Range for Healthy Individuals
For most healthy adults, a normal ejection fraction typically falls within the range of 50% to 70%. This means that with each heartbeat, the left ventricle effectively pumps out at least half of the blood it contains, and up to 70%. An EF in this range indicates that the heart is functioning efficiently and is able to meet the body’s oxygen and nutrient demands.
Factors Influencing Ejection Fraction
While the 50-70% range is standard, it’s important to acknowledge that individual EF values can fluctuate. Certain physiological factors can influence EF:
- Age: As individuals age, some slight decline in cardiac efficiency, and therefore EF, may occur naturally. However, significant drops are not considered normal aging.
- Sex: There can be minor differences in average EF between men and women, though the healthy range remains largely consistent.
- Physical Fitness: Highly conditioned athletes often exhibit higher than average EFs, as their hearts are trained to pump blood more efficiently.
- Pregnancy: During pregnancy, the heart works harder to supply blood to both the mother and the fetus, which can lead to temporary increases in cardiac output and potentially affect EF measurements.
It is crucial to remember that these factors influence the expected range, but a deviation outside the 50-70% window, even within these contexts, warrants medical evaluation.
Understanding Lower Ejection Fraction Values
An ejection fraction below the normal range is a key indicator of reduced heart function. The severity of heart disease is often categorized based on the degree of EF reduction.
- Mildly Reduced EF (40-49%): This range can suggest early signs of heart muscle weakness or damage.
- Moderately Reduced EF (30-39%): This indicates a more significant impairment in the heart’s pumping ability.
- Severely Reduced EF (<30%): An EF in this range signifies severely weakened heart muscle and a high risk of heart failure and other complications.
What About Ejection Fraction Above the Normal Range?
While less common than low EF, an ejection fraction that is consistently above the normal range can also indicate underlying issues. This might be seen in conditions like hypertrophic cardiomyopathy, where the heart muscle thickens, or in certain types of heart valve disease. In these cases, the heart might be overworking to compensate for a problem, leading to an artificially high EF. However, a slightly elevated EF in an otherwise healthy individual, especially an athlete, is generally not a cause for concern.
Conditions Affecting Ejection Fraction
A reduced ejection fraction is a hallmark of several cardiovascular conditions that impair the heart’s ability to pump blood effectively. Identifying these conditions is paramount for timely intervention and management.
Heart Failure (Heart Muscle Weakness)
Heart failure is a chronic condition where the heart cannot pump blood as well as it should. It can affect one or both sides of the heart. There are two main types of heart failure, often distinguished by their EF:
- Heart Failure with Reduced Ejection Fraction (HFrEF): This is characterized by an ejection fraction of 40% or less. In HFrEF, the left ventricle is weakened and enlarged, struggling to contract forcefully enough to pump an adequate amount of blood to the body. Common causes include coronary artery disease, high blood pressure, heart attacks, and viral infections of the heart.
- Heart Failure with Preserved Ejection Fraction (HFpEF): In this type, the ejection fraction is 50% or higher, but the heart muscle is still stiff and cannot relax properly to fill with adequate blood during diastole. While EF is preserved, the overall pumping function is still compromised due to impaired filling. HFpEF is more common in older adults and is often associated with conditions like hypertension, diabetes, and obesity.
Valvular Heart Disease
The heart valves are critical for ensuring unidirectional blood flow. When these valves become damaged or diseased, they can impede blood flow or allow blood to leak backward, placing extra strain on the heart muscle.
- Stenosis: If a valve narrows (stenosis), the heart has to pump harder to push blood through the constricted opening. This increased workload can eventually lead to weakening of the heart muscle and a reduction in EF.
- Regurgitation (Insufficiency): If a valve doesn’t close properly, blood can leak backward into the chamber it just left (regurgitation). This means that less blood is effectively pumped forward with each beat, potentially leading to a lower EF. Conditions like mitral valve regurgitation and aortic valve regurgitation are common examples.
Cardiomyopathy
Cardiomyopathy refers to diseases of the heart muscle itself. These conditions can cause the heart muscle to become enlarged, thickened, or rigid, affecting its ability to pump blood.
- Dilated Cardiomyopathy: The heart chambers, particularly the left ventricle, enlarge, and the heart muscle weakens, leading to a significantly reduced EF.
- Hypertrophic Cardiomyopathy: The heart muscle thickens abnormally, which can obstruct blood flow out of the ventricle and sometimes lead to a high EF if the muscle is overly forceful, or a reduced EF if the thickening impairs filling and contraction.
- Restrictive Cardiomyopathy: The heart muscle becomes stiff, hindering its ability to relax and fill with blood, which can affect overall pumping efficiency, though EF might appear normal or mildly reduced in some cases.
Other Contributing Factors
Several other factors can contribute to or exacerbate a reduced ejection fraction:
- Coronary Artery Disease (CAD): Blockages in the coronary arteries reduce blood flow to the heart muscle. If enough heart muscle is damaged or starved of oxygen (due to a heart attack, for example), its pumping ability can be compromised, leading to a lower EF.
- Hypertension (High Blood Pressure): Chronically high blood pressure forces the heart to work harder to pump blood against increased resistance. Over time, this can lead to thickening and eventual weakening of the heart muscle, reducing its EF.
- Arrhythmias: Irregular heart rhythms can disrupt the coordinated pumping of the heart, leading to reduced efficiency and a lower EF, especially if the heart rate is too fast or too slow for prolonged periods.
- Congenital Heart Defects: Certain birth defects affecting the heart’s structure can impact its pumping function from birth or later in life, influencing EF.
Implications and Management of Ejection Fraction
An ejection fraction measurement is more than just a number; it’s a critical piece of information that guides diagnosis, treatment strategies, and prognosis for patients with cardiovascular disease. Understanding its implications is vital for both healthcare providers and patients.
Prognostic Value of Ejection Fraction
The ejection fraction is a powerful predictor of a patient’s outlook. A lower EF generally correlates with a poorer prognosis and a higher risk of adverse cardiovascular events, including hospitalization for heart failure and mortality.
- Predicting Heart Failure Progression: A declining EF is often indicative of worsening heart failure, signaling a greater need for intensified medical management.
- Risk Stratification: EF helps physicians stratify patients based on their risk, allowing for tailored treatment plans and more aggressive interventions for those with severely reduced EF.
- Guiding Therapy: Certain treatments for heart failure, such as implantable cardioverter-defibrillators (ICDs) and cardiac resynchronization therapy (CRT), are specifically indicated for patients with a significantly reduced EF.
Treatment Strategies Based on EF
Treatment for conditions affecting ejection fraction is highly individualized and depends on the underlying cause and the severity of EF reduction.
- Medications: A cornerstone of heart failure management, medications aim to improve the heart’s pumping ability, reduce its workload, and manage symptoms. These include ACE inhibitors, beta-blockers, diuretics, ARBs, and ARNIs, often prescribed based on EF levels.
- Lifestyle Modifications: For all patients with cardiovascular conditions, lifestyle changes are crucial. These include adopting a heart-healthy diet, engaging in regular physical activity (as advised by a physician), maintaining a healthy weight, quitting smoking, and managing stress.
- Device Therapy: For individuals with severely reduced EF and specific ECG findings, devices like ICDs can prevent sudden cardiac death by delivering an electrical shock to correct life-threatening arrhythmias. CRT can improve the coordination of the heart’s contractions.
- Revascularization Procedures: For patients with CAD contributing to reduced EF, procedures like angioplasty and bypass surgery can restore blood flow to the heart muscle, potentially improving its function.
- Valve Repair or Replacement: If valvular heart disease is significantly impacting EF, surgical intervention to repair or replace the faulty valve may be necessary to restore normal blood flow.

The Importance of Regular Monitoring
For individuals diagnosed with conditions affecting their ejection fraction, regular monitoring is essential. This typically involves periodic echocardiograms to assess changes in EF, evaluate the effectiveness of treatment, and detect any progression of the underlying disease. Close collaboration with a cardiologist ensures that treatment plans are adjusted as needed to optimize cardiac health and improve quality of life.
In conclusion, a normal ejection fraction of 50-70% signifies a healthy and robust heart. However, understanding the spectrum of EF values, the conditions that can affect it, and the implications for prognosis and treatment is paramount for maintaining cardiovascular well-being. Through accurate measurement, appropriate intervention, and diligent monitoring, individuals can effectively manage conditions that impact their heart’s pumping function.