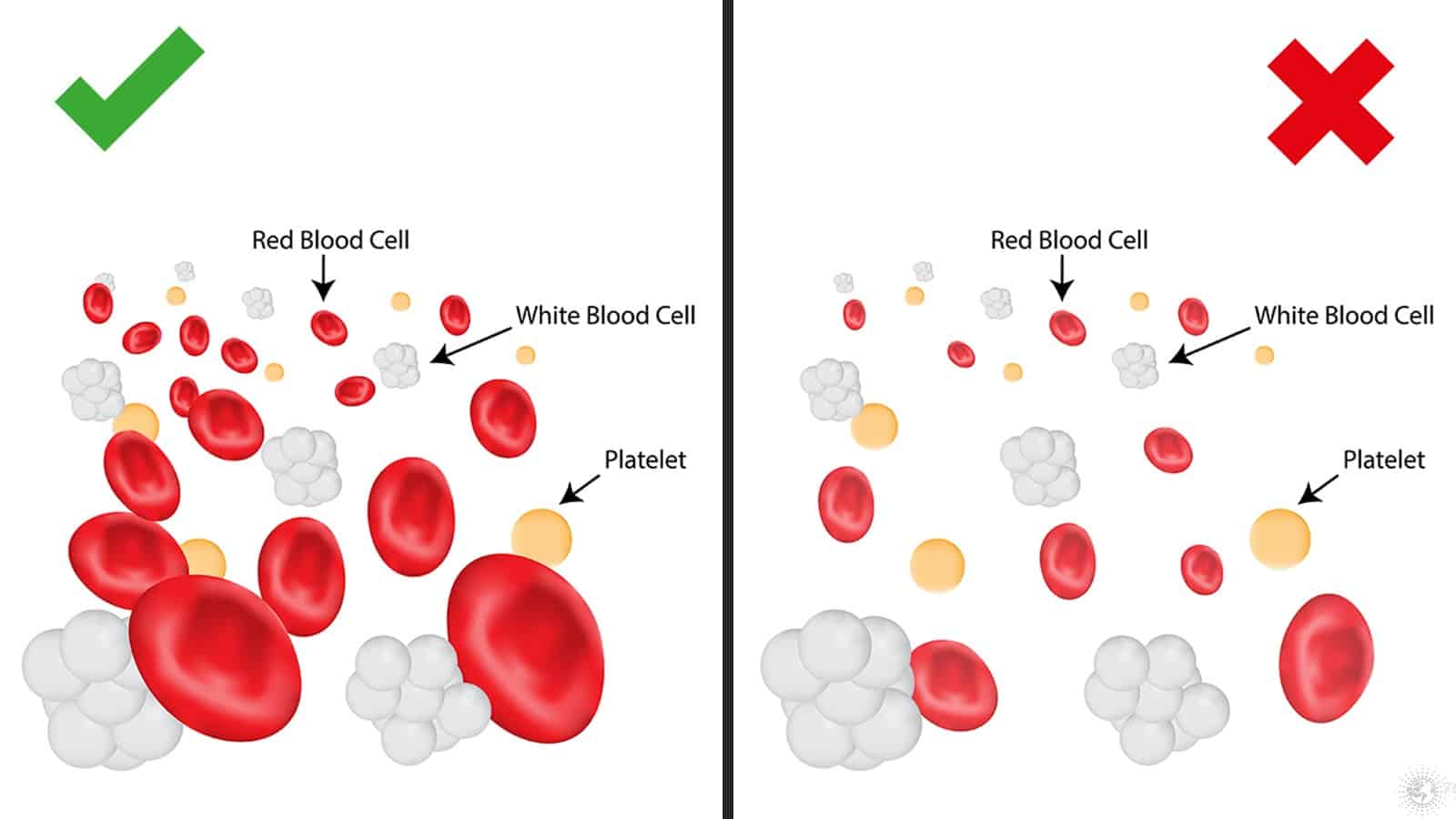
A low Red Blood Cell (RBC) count, also known as anemia, is a medical condition characterized by a deficiency of red blood cells or hemoglobin in the blood. Red blood cells are vital components of our blood, responsible for transporting oxygen from the lungs to all the tissues and organs of the body. Hemoglobin, a protein within red blood cells, is the molecule that binds to oxygen. When RBCs or hemoglobin are insufficient, the body’s cells do not receive enough oxygen, leading to a range of symptoms and potential health complications.
Understanding the implications of a low RBC count is crucial for maintaining overall health. This condition can stem from various underlying causes, each requiring a specific diagnostic approach and treatment plan. From nutritional deficiencies to chronic diseases and genetic predispositions, the reasons behind a low RBC count are diverse. This article will delve into what a low RBC count signifies, explore the common causes, discuss the diagnostic process, and outline the potential treatments and management strategies for this prevalent medical condition.
Understanding Red Blood Cells and Their Function
To fully grasp the significance of a low RBC count, it’s essential to first understand the fundamental role of red blood cells and hemoglobin within the circulatory system.
The Anatomy and Physiology of Red Blood Cells
Red blood cells, also known as erythrocytes, are the most abundant type of blood cell in the human body. They are small, biconcave disc-shaped cells that lack a nucleus in their mature state, a characteristic that allows them to maximize their surface area for gas exchange. The production of red blood cells, a process called erythropoiesis, primarily occurs in the bone marrow. This intricate process is regulated by a hormone called erythropoietin, which is produced by the kidneys in response to low oxygen levels in the blood.
The lifespan of a typical red blood cell is about 120 days. After this period, they are removed from circulation by specialized cells in the spleen and liver. Throughout their existence, red blood cells circulate throughout the body, delivering oxygen and picking up carbon dioxide, a waste product of cellular metabolism, which is then transported back to the lungs for exhalation.
The Critical Role of Hemoglobin
Hemoglobin is the protein contained within red blood cells that is absolutely central to oxygen transport. Each red blood cell contains millions of hemoglobin molecules. Hemoglobin is a complex protein made up of four subunits, each containing a heme group. The iron atom within the heme group is what directly binds to oxygen. When blood passes through the lungs, where oxygen concentration is high, hemoglobin readily binds to oxygen. As the blood circulates to tissues with lower oxygen concentrations, hemoglobin releases its oxygen, fulfilling the body’s metabolic needs.
The amount of hemoglobin in the blood is measured by hemoglobin concentration, which is a key component of a complete blood count (CBC). Low hemoglobin levels directly indicate a reduced capacity for oxygen transport, regardless of the actual number of red blood cells. This is why anemia is often described in terms of low hemoglobin.
Normal RBC Count and Hemoglobin Levels
The normal range for RBC count and hemoglobin levels can vary slightly depending on age, sex, and laboratory reference ranges. However, general guidelines are established for healthy adults.
- Red Blood Cell Count (RBC): For adult males, a typical RBC count ranges from 4.7 to 6.1 million cells per microliter (µL). For adult females, the range is generally 4.2 to 5.4 million cells per µL.
- Hemoglobin (Hgb): For adult males, normal hemoglobin levels are usually between 13.8 to 17.2 grams per deciliter (g/dL). For adult females, the range is typically 12.1 to 15.1 g/dL.
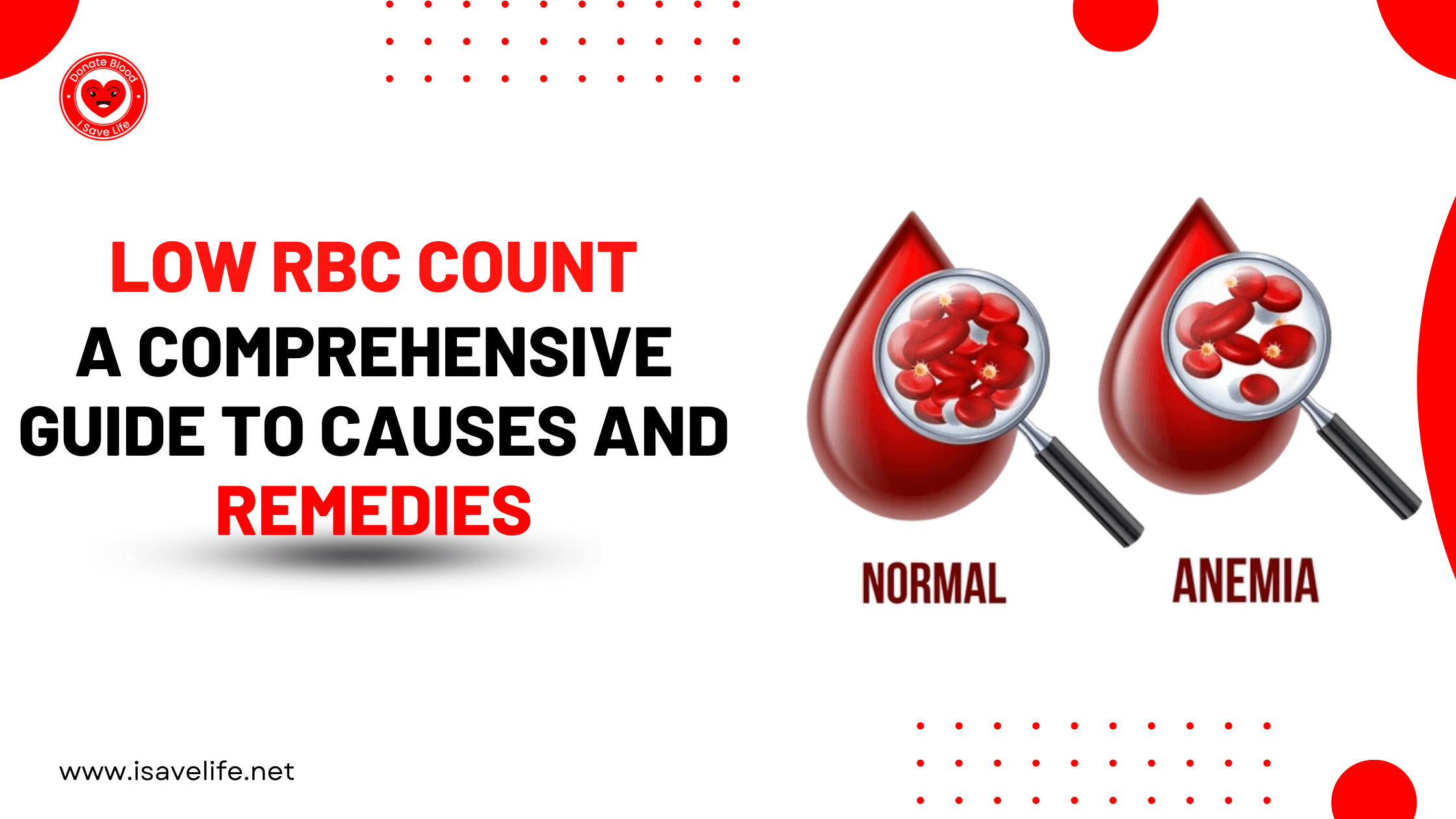
A low RBC count or hemoglobin level below these established ranges is generally indicative of anemia. It’s important to note that these are general ranges, and a healthcare professional will interpret these values in the context of an individual’s overall health status and medical history.
Causes of Low RBC Count (Anemia)
A low RBC count, or anemia, is not a disease in itself but rather a symptom of an underlying issue. The causes are varied and can be broadly categorized into three main groups: decreased production of red blood cells, increased destruction of red blood cells, and blood loss.
Decreased Red Blood Cell Production
This category encompasses conditions where the bone marrow is not producing enough red blood cells to maintain adequate levels.
-
Nutritional Deficiencies:
- Iron Deficiency: Iron is a critical component of hemoglobin. Insufficient iron intake through diet or impaired iron absorption can lead to iron-deficiency anemia, the most common type of anemia worldwide. Factors contributing to this include inadequate dietary iron, heavy menstrual bleeding in women, and gastrointestinal issues that hinder iron absorption.
- Vitamin B12 Deficiency: Vitamin B12 is essential for the synthesis of DNA, a process vital for red blood cell maturation. Deficiency can result in megaloblastic anemia, characterized by abnormally large and immature red blood cells. This deficiency can arise from dietary insufficiency (especially in vegans), pernicious anemia (an autoimmune condition affecting B12 absorption), or certain gastrointestinal surgeries.
- Folate (Folic Acid) Deficiency: Similar to Vitamin B12, folate is crucial for DNA synthesis and red blood cell production. Folate deficiency also leads to megaloblastic anemia. Causes include inadequate dietary intake, increased demand during pregnancy, and certain medical conditions or medications.
-
Bone Marrow Disorders: The bone marrow is the factory for red blood cells. Any condition that impairs its function can lead to anemia.
- Aplastic Anemia: This is a rare but serious condition where the bone marrow fails to produce enough blood cells, including red blood cells, white blood cells, and platelets. It can be caused by autoimmune disorders, exposure to toxins or radiation, viral infections, or be idiopathic (unknown cause).
- Myelodysplastic Syndromes (MDS): These are a group of disorders where the bone marrow produces abnormal blood cells that are often not functional and are destroyed prematurely. MDS can progress to acute myeloid leukemia.
- Leukemia and Lymphoma: Cancers of the blood and lymphatic system can infiltrate the bone marrow, disrupting normal red blood cell production.
-
Chronic Diseases and Inflammation:
- Anemia of Chronic Disease (ACD): This type of anemia is commonly associated with chronic inflammatory conditions such as rheumatoid arthritis, inflammatory bowel disease, chronic infections (like HIV), and certain cancers. The inflammation can interfere with iron metabolism and the body’s ability to use iron for red blood cell production. It can also lead to a shortened red blood cell lifespan.
- Kidney Disease: The kidneys produce erythropoietin (EPO), the hormone that stimulates red blood cell production. In chronic kidney disease, the production of EPO declines, leading to a reduced number of red blood cells.
Increased Red Blood Cell Destruction (Hemolytic Anemias)
In hemolytic anemias, red blood cells are destroyed faster than the bone marrow can replace them.
-
Inherited Conditions:
- Sickle Cell Anemia: This is a genetic disorder where red blood cells have an abnormal, sickle shape, making them rigid and prone to breaking apart and blocking blood flow.
- Thalassemia: This is a group of inherited blood disorders characterized by the body’s inability to produce sufficient hemoglobin, leading to reduced red blood cell production and increased destruction.
- Hereditary Spherocytosis: In this condition, red blood cells are abnormally spherical and fragile, leading to their premature destruction in the spleen.
-
Acquired Conditions:
- Autoimmune Hemolytic Anemia: The body’s immune system mistakenly attacks and destroys its own red blood cells.
- Infections: Certain infections, such as malaria, can directly infect and destroy red blood cells.
- Medication-Induced Hemolysis: Some medications can trigger an immune response that leads to the destruction of red blood cells.
- Mechanical Damage: In rare cases, artificial heart valves or other mechanical devices can damage red blood cells as they pass through.
Blood Loss
Significant or chronic blood loss can deplete the body’s red blood cell reserves.
- Acute Blood Loss: This can occur due to trauma, surgery, or sudden gastrointestinal bleeding (e.g., from a ruptured ulcer or diverticulitis). The body can initially compensate by releasing stored red blood cells, but significant or rapid loss will lead to a low RBC count.
- Chronic Blood Loss: This is often less obvious and can occur over a long period. Common sources include:
- Gastrointestinal Bleeding: This can be caused by peptic ulcers, gastritis, colon polyps, colorectal cancer, or hemorrhoids.
- Menorrhagia (Heavy Menstrual Bleeding): Women experiencing very heavy periods can lose a significant amount of iron and red blood cells over time.
- Frequent Blood Donation: While beneficial for recipients, very frequent donations without adequate iron replenishment can lead to low iron stores and subsequent anemia.
Diagnosis and Symptoms of Low RBC Count
Diagnosing a low RBC count involves a combination of symptom assessment, physical examination, and laboratory tests. Identifying the underlying cause is paramount for effective treatment.
Recognizing the Symptoms
The symptoms of a low RBC count can vary in severity and may not always be immediately apparent, especially in mild cases. When symptoms do occur, they are generally related to the body’s reduced oxygen-carrying capacity.
- Fatigue and Weakness: This is one of the most common and prominent symptoms. Feeling persistently tired, lacking energy, and experiencing generalized weakness are hallmarks of anemia.
- Pale Skin (Pallor): Reduced hemoglobin, which gives blood its red color, can lead to a noticeable paleness of the skin, as well as the lining of the eyelids and nail beds.
- Shortness of Breath (Dyspnea): The body struggles to get enough oxygen to the tissues, leading to a feeling of breathlessness, especially during exertion.
- Dizziness or Lightheadedness: Insufficient oxygen supply to the brain can cause feelings of dizziness, unsteadiness, or lightheadedness.
- Headaches: Reduced oxygen to the brain can also manifest as persistent or recurring headaches.
- Cold Hands and Feet: Poor circulation due to a reduced oxygen supply can lead to extremities feeling unusually cold.
- Rapid or Irregular Heartbeat (Palpitations): The heart may beat faster or irregularly in an attempt to compensate for the reduced oxygen-carrying capacity of the blood, trying to circulate the available oxygen more efficiently.
- Chest Pain: In severe cases, the heart may have to work harder, leading to chest pain, particularly in individuals with pre-existing heart conditions.
- Brittle Nails and Hair Loss: Nutritional deficiencies, particularly iron deficiency, can affect the health of nails and hair.
- Sore or Swollen Tongue (Glossitis) and Cracks at the Corners of the Mouth (Angular Cheilitis): These can be symptoms of certain types of anemia, particularly those related to B12 or folate deficiency.
Diagnostic Tests
A comprehensive diagnostic approach is crucial to accurately identify anemia and its root cause.
-
Complete Blood Count (CBC): This is the primary blood test used to diagnose anemia. A CBC measures:
- Red Blood Cell Count (RBC): The total number of red blood cells per unit volume of blood.
- Hemoglobin (Hgb): The amount of hemoglobin in the blood.
- Hematocrit (Hct): The percentage of blood volume occupied by red blood cells.
- Mean Corpuscular Volume (MCV): The average size of red blood cells. This helps classify anemia into microcytic (small cells), normocytic (normal size), or macrocytic (large cells).
- Mean Corpuscular Hemoglobin (MCH) and Mean Corpuscular Hemoglobin Concentration (MCHC): These measure the average amount and concentration of hemoglobin within individual red blood cells, helping to determine if the cells are hypochromic (pale).
- Red Cell Distribution Width (RDW): This measures the variation in the size of red blood cells. An elevated RDW can indicate the presence of different-sized red blood cells, common in nutritional deficiencies.
-
Peripheral Blood Smear: A microscopic examination of a blood sample allows for detailed observation of the size, shape, and appearance of red blood cells, as well as other blood cells. This can help identify specific abnormalities indicative of certain types of anemia.
-
Reticulocyte Count: Reticulocytes are immature red blood cells. A reticulocyte count measures the bone marrow’s response to anemia. A low reticulocyte count suggests the bone marrow is not producing enough red blood cells, while a high count indicates the bone marrow is trying to compensate for blood loss or destruction.
-
Iron Studies: These tests measure the body’s iron levels:
- Serum Iron: The amount of iron circulating in the blood.
- Ferritin: A protein that stores iron, indicating the body’s iron stores. Low ferritin is a sensitive indicator of iron deficiency.
- Total Iron-Binding Capacity (TIBC): Measures the blood’s capacity to bind iron, which can be elevated in iron deficiency.
- Transferrin Saturation: The percentage of iron-binding sites on transferrin (a protein that transports iron) that are occupied by iron.
-
Vitamin B12 and Folate Levels: Blood tests to measure the levels of these essential vitamins are crucial for diagnosing megaloblastic anemias.
-
Tests for Hemolysis: If hemolytic anemia is suspected, further tests may include:
- Lactate Dehydrogenase (LDH): An enzyme released when red blood cells are destroyed.
- Bilirubin: A byproduct of red blood cell breakdown.
- Haptoglobin: A protein that binds to free hemoglobin released from destroyed red blood cells. Low levels indicate increased hemolysis.
- Direct Antiglobulin Test (DAT) or Coombs Test: Used to detect antibodies attached to red blood cells, suggestive of autoimmune hemolytic anemia.
-
Bone Marrow Biopsy: In complex or persistent cases, a bone marrow biopsy may be performed to directly examine the bone marrow’s cellularity and cellular morphology, helping to diagnose bone marrow disorders, leukemia, or aplastic anemia.
-
Tests for Blood Loss: If blood loss is suspected, investigations might include fecal occult blood tests (to detect hidden blood in stool) or endoscopic procedures (gastroscopy, colonoscopy) to identify the source of bleeding in the gastrointestinal tract.
Treatment and Management of Low RBC Count
The treatment and management of a low RBC count are entirely dependent on the underlying cause. The goal is to address the root problem to restore normal red blood cell production, reduce destruction, or replenish lost blood.
Addressing the Underlying Cause
-
Nutritional Supplementation:
- Iron Supplements: For iron-deficiency anemia, oral iron supplements (ferrous sulfate, ferrous gluconate, ferrous fumarate) are the first line of treatment. In severe cases or when oral absorption is poor, intravenous iron infusions may be necessary. Dietary changes to increase iron-rich foods (red meat, leafy greens, beans) are also recommended.
- Vitamin B12 and Folate Supplements: For deficiencies, oral or injectable supplements of Vitamin B12 and folic acid are prescribed. Dietary adjustments to include foods rich in these vitamins (dairy products, eggs, meat for B12; leafy greens, legumes, fortified cereals for folate) are also important.
-
Treating Chronic Diseases and Inflammation: Managing the underlying chronic condition is crucial. This might involve medications to control inflammation (e.g., in autoimmune diseases), antibiotics for infections, or specific treatments for kidney disease.
-
Managing Bone Marrow Disorders: Treatment for bone marrow disorders varies widely and may include:
- Medications: Immunosuppressive therapy for aplastic anemia, hypomethylating agents or chemotherapy for MDS, and targeted therapies for leukemia.
- Blood Transfusions: To temporarily increase RBC levels and manage symptoms.
- Bone Marrow Transplantation: In severe cases, a bone marrow transplant may be considered as a curative option.
-
Treating Hemolytic Anemias:
- Medications: Steroids (like prednisone) to suppress the immune system in autoimmune hemolytic anemia. Other immunosuppressants may be used if steroids are ineffective.
- Splenectomy: In some cases of severe hemolytic anemia where the spleen is overactive in destroying red blood cells, surgical removal of the spleen may be considered.
- Treating Infections: Addressing and eradicating underlying infections that cause hemolysis.
-
Managing Blood Loss:
- Stopping the Bleeding: This is the primary focus. Depending on the source, it may involve medical or surgical interventions, such as endoscopic cauterization of ulcers, surgical repair of bleeding vessels, or treatments for heavy menstrual bleeding (e.g., hormonal therapy, surgical procedures).
- Iron Supplementation: To replenish iron stores lost due to chronic bleeding.
Symptomatic Relief and Supportive Care
- Blood Transfusions: In cases of severe anemia with significant symptoms or when immediate improvement is needed (e.g., before surgery), blood transfusions can quickly raise RBC and hemoglobin levels, providing symptomatic relief.
- Erythropoiesis-Stimulating Agents (ESAs): These medications, such as epoetin alfa, mimic erythropoietin and stimulate the bone marrow to produce more red blood cells. They are often used in anemia related to chronic kidney disease or certain cancer treatments.
- Lifestyle Modifications:
- Diet: Emphasizing a balanced diet rich in iron, B12, and folate is beneficial for all types of anemia.
- Rest and Energy Conservation: Managing fatigue by prioritizing rest and pacing activities can improve quality of life.
- Avoiding Strenuous Activity: During periods of significant anemia, avoiding activities that exacerbate shortness of breath or fatigue is important.
Long-Term Management and Monitoring
Following a diagnosis of low RBC count, ongoing monitoring is essential to ensure the effectiveness of treatment and to detect any recurrence or complications. This typically involves regular blood tests (CBC, iron studies, etc.) and follow-up appointments with a healthcare provider. For individuals with chronic conditions, a long-term management plan will be established, often in collaboration with specialists. Understanding the specific cause of anemia empowers patients to play an active role in their health management, leading to better outcomes and an improved quality of life.