The human body is a marvel of intricate biological systems, and understanding its various components and potential ailments is crucial for maintaining well-being. Among the many conditions that can affect us, those involving the urinary tract are quite common. One such condition, often experienced acutely and causing significant discomfort, is acute cystitis. This article aims to demystify acute cystitis, exploring its nature, causes, symptoms, diagnostic approaches, and management strategies. By shedding light on this prevalent health concern, we can foster greater awareness and empower individuals to seek appropriate care.
Understanding Acute Cystitis
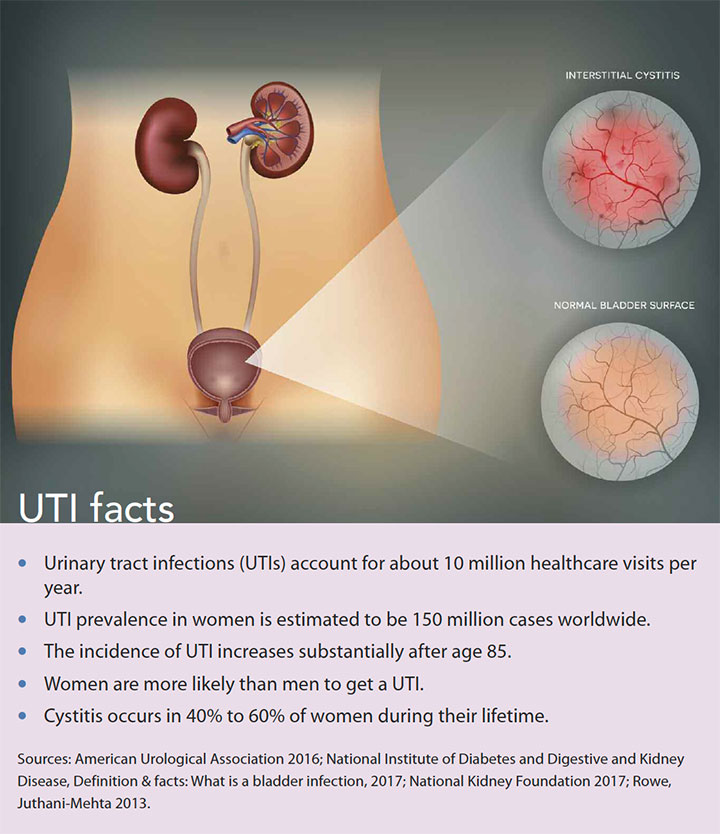
At its core, acute cystitis refers to a sudden and often intense inflammation of the urinary bladder. The bladder, a hollow, muscular organ situated in the pelvis, serves as a reservoir for urine produced by the kidneys. When acute cystitis occurs, the lining of the bladder becomes irritated and inflamed, leading to a characteristic set of symptoms. The term “acute” signifies that the onset is relatively rapid and the duration is typically short-lived, though it can recur.
The Anatomy and Function of the Bladder
To fully grasp acute cystitis, a basic understanding of the bladder’s anatomy and function is beneficial. The bladder is roughly pear-shaped and is composed of several layers, including an inner lining called the urothelium. This specialized tissue is designed to withstand the corrosive effects of urine. The bladder’s primary function is to store urine, a waste product filtered from the blood by the kidneys. Muscles within the bladder wall, known as the detrusor muscles, contract to expel urine through the urethra, the tube that carries urine from the bladder out of the body. The coordinated action of these muscles, along with sphincters that control the flow of urine, ensures continence.
The Pathophysiology of Inflammation
Inflammation, in general, is the body’s natural response to injury or infection. In the case of acute cystitis, the inflammation is typically triggered by the presence of harmful microorganisms within the bladder. When these pathogens invade the bladder, they can disrupt the integrity of the urothelium, leading to cellular damage and the release of inflammatory mediators. These mediators, such as cytokines and prostaglandins, recruit immune cells to the site of infection, further contributing to the inflammatory process. This cascade of events results in the characteristic pain, burning, and frequent urination associated with cystitis. The inflammation can cause the bladder wall to become edematous (swollen) and hypersensitive, leading to bladder spasms and an increased urge to urinate.
Causes and Risk Factors of Acute Cystitis
The primary driver of acute cystitis is bacterial infection, though other factors can contribute to its development or increase an individual’s susceptibility. Identifying these causes and risk factors is crucial for prevention and effective treatment.
Bacterial Infections: The Primary Culprit
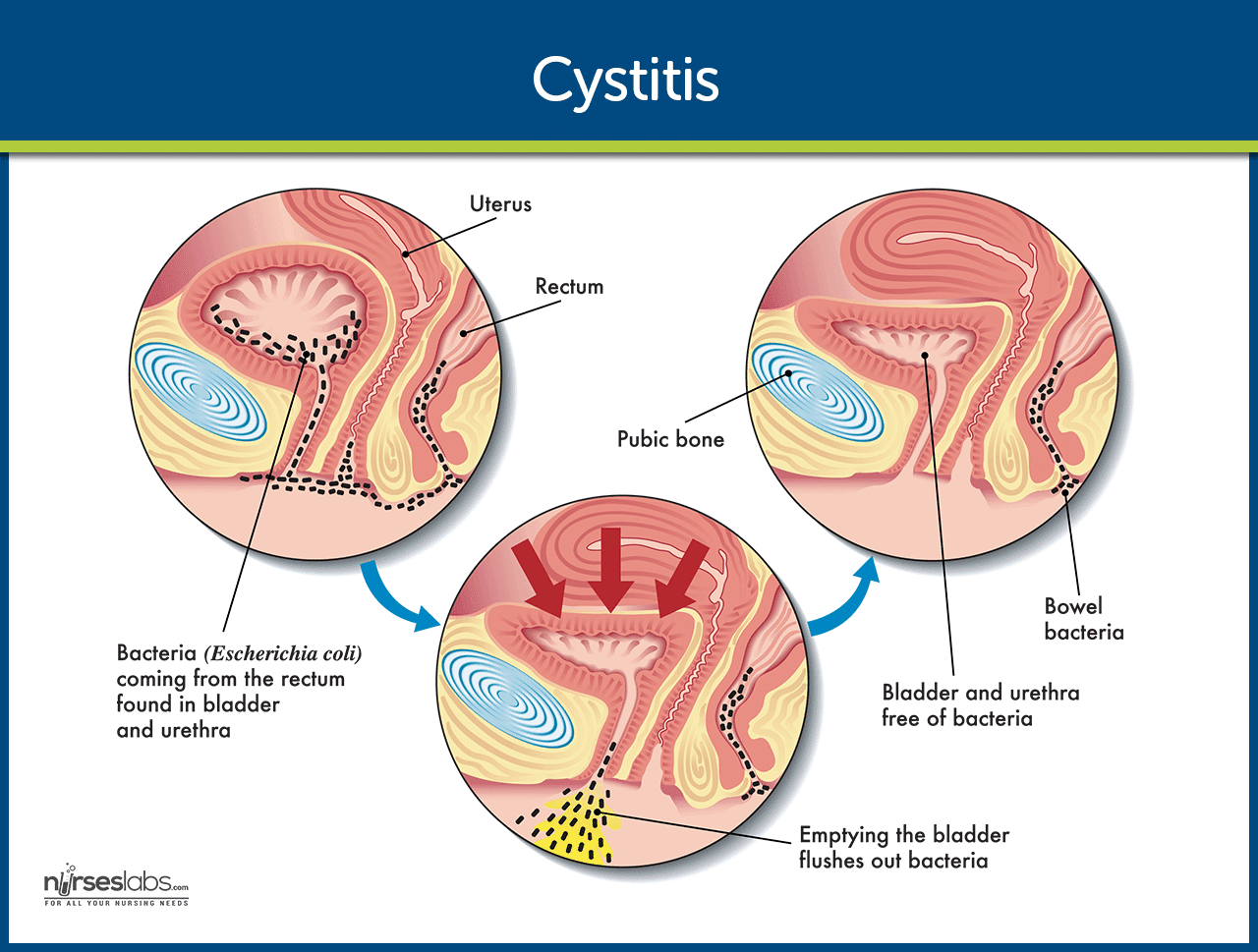
The vast majority of acute cystitis cases are caused by bacteria that ascend from the perineal area (the region between the anus and the genitals) into the urethra and subsequently into the bladder. Escherichia coli (E. coli), a common bacterium found in the gastrointestinal tract, is responsible for approximately 80-90% of uncomplicated cystitis cases in women. Other bacteria that can cause cystitis include Staphylococcus saprophyticus, Klebsiella pneumoniae, and Proteus mirabilis. These bacteria can adhere to the urothelium, multiply, and trigger the inflammatory response.
Anatomical and Physiological Factors
Certain anatomical and physiological characteristics can predispose individuals to acute cystitis. In women, the shorter urethra compared to men provides a more direct pathway for bacteria to reach the bladder. Furthermore, the proximity of the urethral opening to the anus in women increases the likelihood of fecal bacteria entering the urinary tract. During sexual intercourse, friction can help propel bacteria into the urethra.
Behavioral and Lifestyle Factors
Several behavioral and lifestyle choices can influence the risk of developing acute cystitis. These include:
- Incomplete Bladder Emptying: Not fully emptying the bladder can leave residual urine, which can serve as a breeding ground for bacteria. This can be due to various reasons, including holding urine for extended periods or conditions that impair bladder emptying.
- Hygiene Practices: Inadequate hygiene can contribute to the spread of bacteria. Conversely, excessive or harsh douching can disrupt the natural flora of the vagina, potentially increasing the risk of urinary tract infections.
- Sexual Activity: As mentioned, sexual intercourse can introduce bacteria into the urethra. Some women experience “honeymoon cystitis,” which is linked to increased frequency of intercourse.
- Use of Certain Contraceptives: Diaphragms and spermicidal agents can alter the vaginal flora and are associated with an increased risk of cystitis.
- Dehydration: Insufficient fluid intake can lead to more concentrated urine, which may irritate the bladder lining and reduce the flushing effect that helps clear bacteria.
- Irritating Products: The use of certain feminine hygiene products, scented soaps, bubble baths, or bath oils can irritate the urethra and bladder, making them more susceptible to infection.
Other Contributing Factors
Beyond the common causes, other factors can play a role in acute cystitis:
- Catheterization: Indwelling urinary catheters, used to drain the bladder, are a significant risk factor for catheter-associated urinary tract infections (CAUTIs), which are a form of cystitis.
- Medical Conditions: Certain medical conditions can increase the risk of cystitis, including diabetes (due to impaired immune function and increased glucose in urine), kidney stones (which can obstruct urine flow and promote bacterial growth), and conditions that affect the immune system.
- Menopause: In postmenopausal women, declining estrogen levels can lead to changes in the vaginal and urethral tissues, making them more vulnerable to bacterial colonization and infection.
- Pregnancy: Hormonal changes during pregnancy can make women more susceptible to urinary tract infections.
- Antibiotic Use: While antibiotics are used to treat cystitis, prolonged or inappropriate antibiotic use can disrupt the body’s natural bacterial balance, potentially leading to the overgrowth of certain pathogens.
Symptoms and Diagnosis of Acute Cystitis
Recognizing the symptoms of acute cystitis is the first step toward seeking timely medical attention. A healthcare professional will then employ various diagnostic methods to confirm the diagnosis and identify the causative agent.
Recognizing the Hallmarks of Cystitis
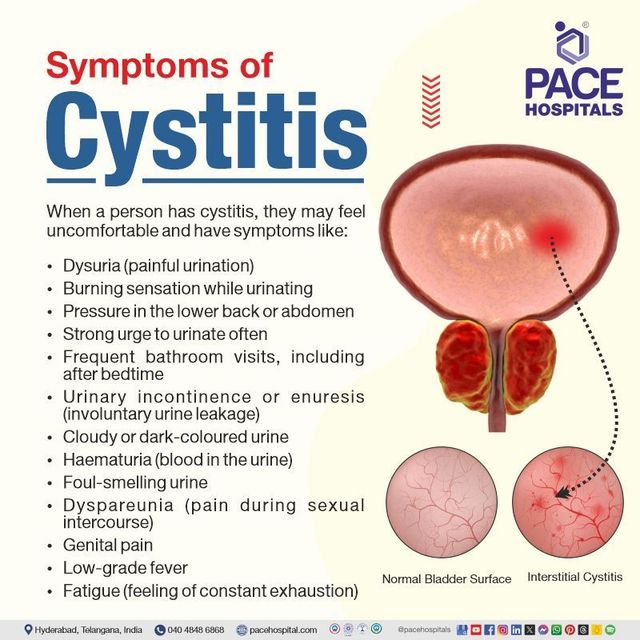
The symptoms of acute cystitis typically appear suddenly and can significantly impact an individual’s daily life. Common signs and symptoms include:
- Frequent Urination (Frequency): An overwhelming and persistent urge to urinate, often passing only small amounts of urine each time.
- Pain or Burning During Urination (Dysuria): A stinging, burning, or painful sensation when urine passes through the urethra. This is often the most prominent and bothersome symptom.
- Urgency: A sudden, intense need to urinate that is difficult to postpone.
- Suprapubic Pain: Discomfort or pressure in the lower abdomen, above the pubic bone.
- Cloudy or Strong-Smelling Urine: The urine may appear murky or have an unusually strong, unpleasant odor.
- Blood in the Urine (Hematuria): Visible blood in the urine can range from pink or reddish discoloration to frank blood clots.
- General Malaise: Some individuals may experience fatigue, mild fever, or a general feeling of being unwell.
It is important to note that not everyone will experience all of these symptoms, and their intensity can vary.
The Diagnostic Process
When a patient presents with symptoms suggestive of acute cystitis, a healthcare provider will typically follow a structured diagnostic approach:
Medical History and Physical Examination
The initial step involves a thorough medical history. The physician will inquire about the onset and nature of symptoms, any recent sexual activity, fluid intake, personal or family history of UTIs, and the presence of any underlying medical conditions. A physical examination may be performed to assess for tenderness in the lower abdomen or flank, although this is often not a primary diagnostic tool for uncomplicated cystitis.
Urinalysis: The Cornerstone of Diagnosis
A urinalysis is a crucial laboratory test performed on a urine sample. It involves several components:
- Macroscopic Examination: Assessing the color, clarity, and odor of the urine.
- Chemical Examination (Dipstick Test): This involves dipping a chemically treated strip into the urine to detect the presence of certain substances. Key findings suggestive of infection include:
- Leukocyte Esterase: An enzyme released by white blood cells (leukocytes), indicating inflammation and the presence of infection.
- Nitrites: Bacteria can convert nitrates (normally present in urine) into nitrites. A positive nitrite test is highly suggestive of a bacterial UTI.
- Microscopic Examination: Under a microscope, the urine sample is examined for the presence of:
- White Blood Cells (Pyuria): An elevated number of white blood cells indicates inflammation and infection.
- Red Blood Cells (Hematuria): Presence of red blood cells, confirming blood in the urine.
- Bacteria: Direct visualization of bacteria can confirm their presence.
Urine Culture and Sensitivity Testing
If the urinalysis is suggestive of a bacterial infection, a urine culture and sensitivity test is often performed. The urine sample is sent to a laboratory where it is cultured on a growth medium to identify the specific type of bacteria causing the infection. Once identified, the bacteria are then tested against a panel of antibiotics to determine which ones are most effective in killing them. This “sensitivity” information is vital for guiding antibiotic treatment and preventing the development of antibiotic resistance.
Imaging Studies (When Necessary)
In most cases of uncomplicated acute cystitis, imaging studies are not required for diagnosis. However, they may be ordered if there are recurrent infections, suspicion of complications (such as kidney involvement or structural abnormalities), or in individuals with underlying risk factors. These may include:
- Kidney, Ureter, and Bladder (KUB) X-ray: Can help identify kidney stones.
- Ultrasound of the Kidneys and Bladder: Can visualize the kidneys, bladder, and surrounding structures, detecting abnormalities like stones, tumors, or signs of obstruction.
- Computed Tomography (CT) Scan: Provides more detailed cross-sectional images and is useful for evaluating more complex cases or complications.
- Cystoscopy: A procedure where a thin, flexible tube with a camera (cystoscope) is inserted into the bladder through the urethra to visually inspect the bladder lining. This is typically reserved for recurrent or complicated cases.
Management and Prevention of Acute Cystitis
Effective management of acute cystitis involves alleviating symptoms and eradicating the infection. Preventive measures are also key to reducing the frequency and severity of recurrences.
Treatment Strategies: Antibiotics and Symptom Relief
The primary treatment for acute bacterial cystitis is a course of antibiotics prescribed by a healthcare professional. The choice of antibiotic and the duration of treatment depend on the type of bacteria identified, the severity of symptoms, and any underlying medical conditions or risk factors.
- Antibiotic Therapy: Common antibiotics used to treat acute cystitis include trimethoprim-sulfamethoxazole, nitrofurantoin, and fosfomycin. For more severe infections or when specific bacteria are involved, other antibiotics such as fluoroquinolones or cephalosporins may be prescribed. It is crucial to complete the entire course of antibiotics as prescribed, even if symptoms improve, to ensure the infection is fully eradicated and to prevent the development of antibiotic resistance.
- Symptom Relief: In addition to antibiotics, measures can be taken to alleviate the discomfort associated with cystitis:
- Pain Relievers: Over-the-counter pain relievers such as ibuprofen or acetaminophen can help manage suprapubic pain and discomfort.
- Urinary Analgesics: Medications like phenazopyridine (available over-the-counter or by prescription) can provide rapid relief from the burning sensation during urination by numbing the urinary tract. It’s important to note that this medication turns urine orange or red and does not treat the infection itself.
- Increased Fluid Intake: Drinking plenty of water helps to flush out the urinary tract, diluting urine and reducing irritation. Aim for clear or pale yellow urine.
- Warm Compresses: Applying a warm compress to the lower abdomen can help soothe bladder spasms and discomfort.
Preventing Recurrent Cystitis
For individuals who experience recurrent bouts of acute cystitis, a proactive approach to prevention is essential. Strategies include:
- Hydration: Maintaining adequate fluid intake throughout the day is paramount.
- Urination Habits:
- Empty the bladder completely every time you urinate.
- Do not hold urine for prolonged periods.
- Urinate soon after sexual intercourse to help flush out any bacteria that may have entered the urethra.
- Hygiene Practices:
- Wipe from front to back after using the toilet to prevent the spread of bacteria from the anus to the urethra.
- Avoid douching and opt for mild, unscented soaps for external cleansing.
- Consider showering instead of bathing, especially if using bubble baths or scented bath products.
- Dietary Considerations: While evidence is mixed, some individuals find that avoiding bladder irritants like caffeine, alcohol, spicy foods, and artificial sweeteners may help.
- Cranberry Products: Some studies suggest that cranberry products (juice or supplements) may help prevent recurrent UTIs by preventing bacteria from adhering to the bladder wall. However, the evidence is not conclusive, and they should not be relied upon as a sole treatment.
- Estrogen Therapy (for postmenopausal women): For women experiencing recurrent UTIs related to menopause, low-dose vaginal estrogen therapy may be recommended by a healthcare provider to restore vaginal health and reduce susceptibility to infection.
- Prophylactic Antibiotics: In cases of frequent and debilitating recurrent UTIs, a healthcare provider may consider a course of low-dose prophylactic antibiotics taken daily or intermittently after sexual intercourse. This is typically a short-term solution and is carefully managed to minimize the risk of antibiotic resistance.
By understanding the causes, symptoms, and effective management strategies for acute cystitis, individuals can better protect their urinary health and seek appropriate care when needed. Prompt diagnosis and treatment are crucial for a swift recovery and for minimizing the risk of complications.