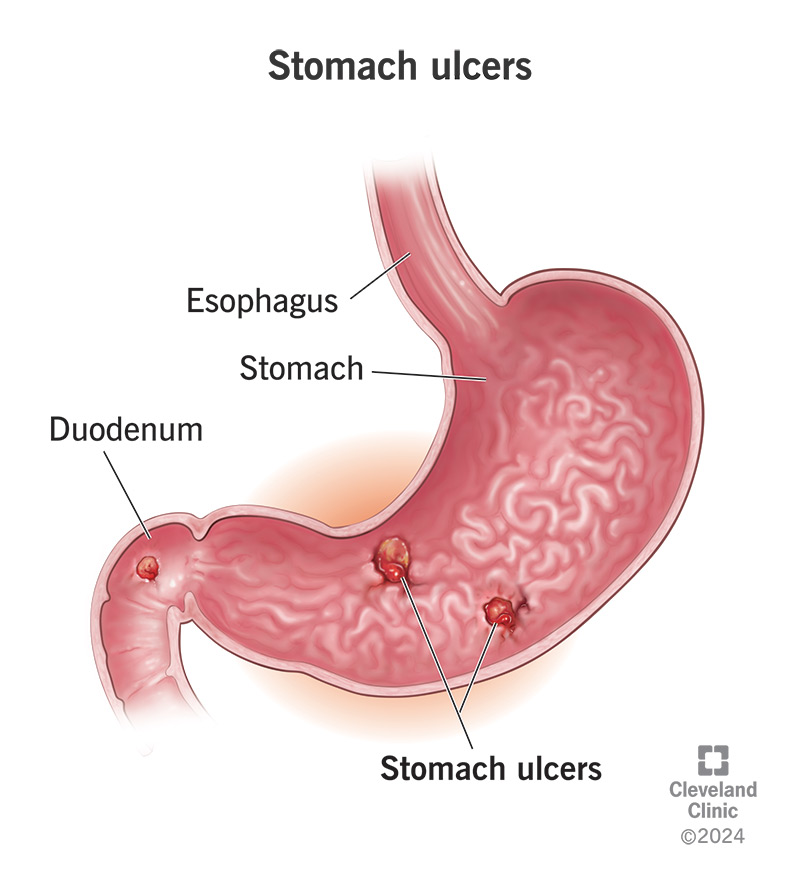
The term “bleeding ulcer” immediately evokes a sense of urgency and medical concern. In essence, it refers to an open sore, typically found in the lining of the stomach or the upper part of the small intestine (the duodenum), that has eroded into a blood vessel. This erosion leads to active bleeding, which can range from a slow, chronic trickle to a sudden, life-threatening hemorrhage. Understanding what a bleeding ulcer is, why it occurs, and its potential consequences is crucial for prompt diagnosis and effective management.
The Nature of Ulcers: From Open Sores to Bleeding Threats
An ulcer itself is a lesion, a damaged area of tissue. In the context of the gastrointestinal (GI) tract, these are commonly known as peptic ulcers. They form when the protective mucosal lining of the stomach or duodenum is compromised, allowing digestive acids and enzymes to damage the underlying tissues.

Understanding the Location and Formation of Peptic Ulcers
- Stomach Ulcers (Gastric Ulcers): These occur within the stomach itself. The stomach lining is normally protected by a thick layer of mucus. However, factors that weaken this defense or increase acid production can lead to the formation of gastric ulcers.
- Duodenal Ulcers: These are the most common type of peptic ulcer and are found in the first part of the small intestine, the duodenum. The duodenum has a slightly different lining than the stomach, but it is also susceptible to acid damage.
- Esophageal Ulcers: Less common, these occur in the esophagus, the tube connecting the throat to the stomach. They are often associated with acid reflux.
The formation of peptic ulcers is a complex process, but two primary culprits are consistently identified: infection with Helicobacter pylori (H. pylori) bacteria and the long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs).
The Role of Helicobacter pylori (H. pylori) Infection
H. pylori is a spiral-shaped bacterium that can colonize the stomach lining. It possesses enzymes that neutralize stomach acid, allowing it to survive and thrive. Over time, H. pylori can trigger inflammation in the stomach lining (gastritis), which can weaken the mucosal barrier. This inflammation makes the lining more vulnerable to the damaging effects of stomach acid and pepsin, a digestive enzyme. The bacterium can also directly damage the cells of the stomach lining, further contributing to ulcer formation. In many cases, H. pylori infection is asymptomatic, but in a significant portion of individuals, it leads to the development of peptic ulcers.
The Impact of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
NSAIDs, a class of medications widely used for pain relief and to reduce inflammation, are also a significant cause of peptic ulcers. Common examples include aspirin, ibuprofen (Advil, Motrin), and naproxen (Aleve). These drugs work by inhibiting enzymes called cyclooxygenases (COX-1 and COX-2). While this inhibition reduces pain and inflammation, it also reduces the production of prostaglandins. Prostaglandins play a crucial role in protecting the stomach lining by increasing mucus production, promoting blood flow to the lining, and reducing acid secretion. When prostaglandin production is suppressed by NSAIDs, the stomach lining becomes more vulnerable to acid damage, leading to ulcer formation. The risk of NSAID-induced ulcers is particularly high with long-term or high-dose use, and in individuals with other risk factors.
Identifying the Signs and Symptoms of a Bleeding Ulcer
The presence of an ulcer may not always be apparent, especially in its early stages. However, when an ulcer begins to bleed, a distinct set of symptoms can emerge, signaling the need for immediate medical attention.
The Subtle and the Severe: Manifestations of Bleeding
The symptoms of a bleeding ulcer can vary greatly depending on the rate and volume of blood loss. Some individuals may experience mild, intermittent bleeding that goes unnoticed for a period, while others can suffer from a sudden, massive hemorrhage.
- Vomiting Blood (Hematemesis): This is a classic sign of upper GI bleeding. The vomited blood can appear bright red if the bleeding is recent and rapid, or it may look like coffee grounds if the blood has been partially digested by stomach acid.
- Bloody or Black, Tarry Stools (Melena): As blood passes through the digestive tract, it undergoes chemical changes. This results in stools that are black, sticky, and have a tar-like appearance and a distinctive foul odor. Melena indicates bleeding in the upper GI tract, including the stomach or duodenum.
- Anemia: Chronic, slow bleeding from an ulcer can lead to a gradual loss of red blood cells. Over time, this can result in iron-deficiency anemia, characterized by fatigue, weakness, pale skin, shortness of breath, and dizziness. The body’s iron stores are depleted as it tries to compensate for the continuous loss of red blood cells.
- Abdominal Pain: While not exclusively a symptom of bleeding, abdominal pain is a common hallmark of ulcers. The pain is often described as a burning or gnawing sensation in the upper abdomen, and it may be exacerbated by an empty stomach and relieved by food or antacids. However, in some cases of bleeding, the pain might be masked by other symptoms.
- Dizziness and Lightheadedness: Significant blood loss can lead to a drop in blood pressure, causing feelings of dizziness, lightheadedness, and even fainting, particularly when standing up.
- Weakness and Fatigue: General weakness and persistent fatigue are common symptoms associated with blood loss, whether it’s acute or chronic.
The Silent Bleeder: When Symptoms are Minimal
It is important to note that some individuals with bleeding ulcers may experience surprisingly few symptoms, especially if the bleeding is slow and intermittent. They might only become aware of the problem when they develop significant anemia or experience a more severe bleeding episode. This highlights the importance of seeking medical advice for persistent or unexplained GI symptoms, even if they seem mild.
Diagnosing the Source: Uncovering the Bleeding Ulcer
When a bleeding ulcer is suspected, a thorough medical evaluation is essential to confirm the diagnosis, identify the underlying cause, and determine the best course of treatment. This typically involves a combination of medical history, physical examination, and diagnostic procedures.
The Crucial Role of Medical History and Physical Examination
A healthcare provider will begin by asking detailed questions about the patient’s symptoms, including their onset, duration, severity, and any factors that seem to exacerbate or alleviate them. They will inquire about:
- The nature of any abdominal pain experienced.
- Any changes in bowel habits, including the appearance of stools.
- Any instances of vomiting, and the appearance of the vomitus.
- The patient’s use of medications, particularly NSAIDs and aspirin.
- Any history of ulcers or other gastrointestinal conditions.
- Family history of GI problems.
A physical examination will involve assessing the patient’s vital signs (blood pressure, heart rate, temperature) and palpating the abdomen to check for tenderness, masses, or other abnormalities. The healthcare provider will also look for signs of anemia, such as pale skin and conjunctiva.
Endoscopic Visualization: The Gold Standard for Diagnosis
The most definitive method for diagnosing a bleeding ulcer and identifying its source is an upper endoscopy, also known as esophagogastroduodenoscopy (EGD). This procedure involves inserting a thin, flexible tube with a camera attached (an endoscope) through the mouth, down the esophagus, into the stomach, and then into the duodenum.
- Visual Inspection: The endoscope allows the physician to directly visualize the lining of the esophagus, stomach, and duodenum. This enables them to identify the presence of ulcers, assess their size and appearance, and importantly, detect active bleeding.
- Biopsy: During the endoscopy, the physician can take small tissue samples (biopsies) from the ulcer and surrounding areas. These biopsies are crucial for testing for H. pylori infection and ruling out other conditions, such as cancer.
- Therapeutic Interventions: In many cases, bleeding ulcers can be treated during the endoscopy. This may involve:
- Injection Therapy: Injecting medications directly into the bleeding site to stop the bleeding.
- Thermal Coagulation: Using heat to seal off bleeding blood vessels.
- Clipping: Applying small metal clips to close off the bleeding vessel.
Imaging Studies: Complementary Diagnostic Tools
While endoscopy is the primary diagnostic tool, other imaging studies may be used in certain situations:
- Barium Swallow/Upper GI Series: This involves swallowing a contrast agent (barium) that coats the lining of the esophagus, stomach, and duodenum. X-rays are then taken to visualize any abnormalities, including ulcers. However, this method is less sensitive than endoscopy for detecting active bleeding and small ulcers.
- CT Scan (Computed Tomography): A CT scan can provide detailed cross-sectional images of the abdomen and can help identify complications of ulcers, such as perforation or bleeding, although it is not the preferred method for directly visualizing the ulcer itself.
Managing the Bleed and Preventing Recurrence
The management of a bleeding ulcer focuses on two primary goals: stopping the active bleeding and preventing it from happening again. The treatment approach will depend on the severity of the bleeding, the underlying cause, and the patient’s overall health.
Immediate Interventions for Active Bleeding
For patients experiencing significant bleeding, immediate medical intervention is critical.
- Intravenous Fluids and Blood Transfusions: Patients who have lost a substantial amount of blood will require intravenous fluids to restore blood volume and potentially blood transfusions to replace lost red blood cells.
- Acid Suppression Therapy: Medications that reduce stomach acid production, such as proton pump inhibitors (PPIs), are crucial. By decreasing acid levels, they create a more favorable environment for healing and can help slow down bleeding. These are often administered intravenously in acute settings.
- Endoscopic Treatment: As mentioned earlier, endoscopy often plays a key role in controlling active bleeding directly.
Addressing the Underlying Cause: Eradicating H. pylori and NSAID Management
- H. pylori Eradication Therapy: If H. pylori infection is identified as the cause of the ulcer, a course of antibiotics, often in combination with a PPI, will be prescribed to eradicate the bacteria. Completing the full course of antibiotics is essential for successful eradication.
- NSAID Discontinuation or Modification: If NSAIDs are contributing to the ulcer, the healthcare provider will advise on discontinuing or reducing their use. For individuals who require NSAIDs for chronic conditions, alternative pain management strategies or the use of COX-2 selective inhibitors (which have a lower risk of GI side effects) may be considered.
Long-Term Strategies for Healing and Prevention
- Continued Acid Suppression: Even after the bleeding is controlled, patients may need to continue taking acid-suppressing medications for a period to allow the ulcer to heal completely.
- Lifestyle Modifications: While not direct causes of ulcers, certain lifestyle factors can exacerbate symptoms and hinder healing. These include smoking, excessive alcohol consumption, and high-stress levels. Quitting smoking, moderating alcohol intake, and implementing stress management techniques can be beneficial.
- Dietary Considerations: While specific diets don’t cause or cure ulcers, some individuals find that avoiding spicy foods, caffeine, and acidic beverages helps to alleviate discomfort.
- Regular Follow-Up: Patients who have experienced a bleeding ulcer will typically require regular follow-up appointments with their healthcare provider to monitor healing, ensure the underlying cause has been addressed, and assess for any signs of recurrence.
In conclusion, a bleeding ulcer is a serious medical condition that arises from the erosion of a blood vessel within a peptic ulcer. Understanding the causes, recognizing the symptoms, and seeking prompt medical diagnosis and treatment are paramount. With appropriate management, most bleeding ulcers can be effectively treated, allowing for healing and a return to good health.